Left ventricular hypertrabeculation/noncompaction is associated with various neuromuscular and other rare genetic disorders. In a 53-year-old man with a Turner mosaic karyotype, regression of left ventricular hypertrabeculation/noncompaction was documented by cardiac magnetic resonance imaging and echocardiography after 7 years. During that time, coronary 3-vessel disease and severe left ventricular dys function developed, necessitating coronary bypass surgery. Postoperatively, left ventricular systolic function recovered to an ejection fraction of 40%. The patient died suddenly 6 months postoperatively. In conclusion, the disappearance of left ventricular hypertrabeculation/noncompaction was most likely due to scar formation.
Left ventricular hypertrabeculation/noncompaction (LVHT) is a rare abnormality characterized by a spongelike meshwork of myocardial interwoven strings distal to the papillary muscles and is frequently associated with various neuromuscular and genetic disorders. The association of LVHT with Turner syndrome has been reported twice. We present the follow-up of 1 of these patients, in whom LVHT regressed.
Case description
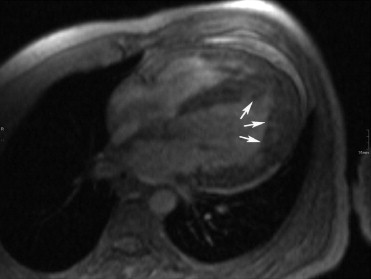
The patient was a 53-year-old man who developed heart failure at age 45 years (August 2003). Because of dwarfism (height 153 cm) and facial dysmorphism, analysis of his karyotype revealed a Turner mosaic karyotype, mos45,X(28)/46,X,+mar(21)/47,X,+2mar(1), confirmed by fluorescence in situ hybridization. Phenotypically, the patient had male genitalia with cryptorchidism, which was operated in early childhood, and hypospadias. Echocardiography revealed a left ventricular ejection fraction of 20% and moderate mitral and mild tricuspid regurgitation. LVHT was suspected echocardiographically in the posterolateral region and was confirmed by cardiac magnetic resonance imaging (CMRI) with a ratio of noncompacted to compacted myocardium >2.3 ( Figure 1 ) . After therapy with lisinopril (40 mg/day) and carvedilol (50 mg/day), the patient’s condition improved, with the left ventricular ejection fraction increasing to normal.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


