9 Diagnostic Coronary Angiography
Coronary Anatomy and Anomalies
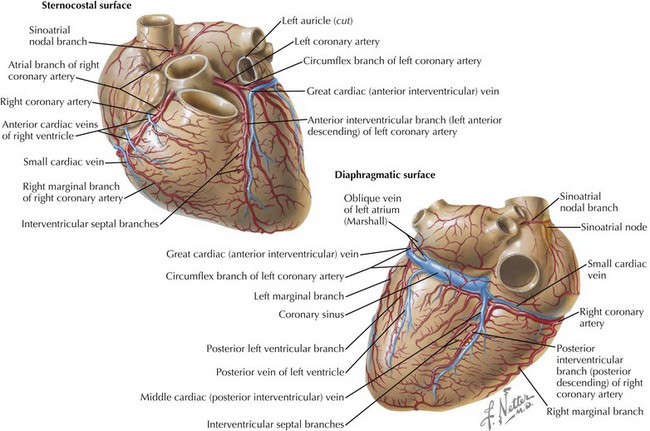
The right coronary artery (RCA) arises from the right coronary sinus and runs in the right atrioventricular groove (Fig. 9-1). Generally, the conus artery and the sinoatrial artery arise from the RCA. In approximately 85% of individuals, the posterior descending coronary artery arises from the RCA (defined as a right dominant coronary circulation). The left main coronary artery arises from the left coronary sinus. Within a few centimeters of its origin, it divides into the left anterior descending (LAD) coronary artery (in the anterior interventricular groove), the left circumflex coronary artery (in the atrioventricular groove), and, in a minority of cases, a ramus intermedius artery.
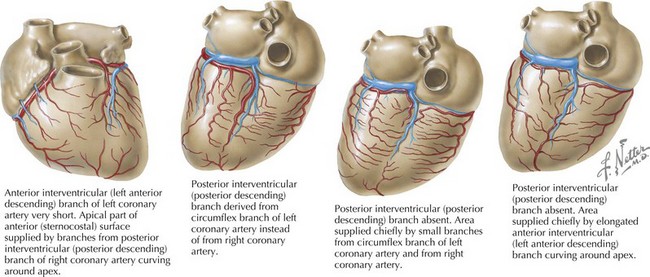
Coronary artery anomalies are found in 1% to 1.5% of individuals (Fig. 9-2), and most of these anomalies are benign. The most common coronary artery anomaly is the presence of separate origins of the LAD and left circumflex arteries from the aorta (i.e., absence of a left main coronary artery), which occurs in 0.4% to 1% of individuals and is occasionally associated with a bicuspid aortic valve. Clinically significant anomalies include origin of a coronary artery from the opposite coronary sinus (e.g., left main artery originating from the right coronary sinus), presence of a single coronary ostium (and hence a single coronary artery), and origin of a coronary artery from the pulmonary artery.
Description of Technique
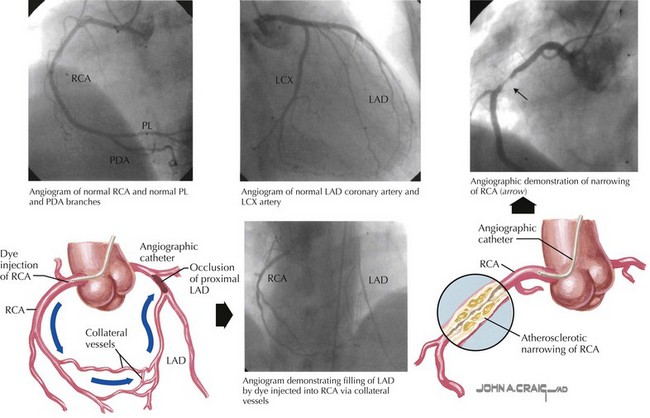
Coronary angiography delineates the course and size of the coronary arteries, identifies coronary anomalies, and provides information on the location and degree of any obstruction (Box 9-1). Coronary angiography is performed by injecting radiopaque contrast dye directly into the ostium of the left and right coronary arteries. Access to the aorta is usually gained via percutaneous puncture of the femoral artery; however, brachial, radial, and axillary arteries can also be used for arterial access. Specific preformed catheters are passed over a guide wire into the aortic root. Selection of the catheter to be used depends on the access site, the coronary artery being investigated, and operator preference. The wire is removed, and the coronary artery is cannulated with fluoroscopic guidance. Contrast dye is injected during cineradiography, while blood pressure and ECG are continually monitored and sequential frames are recorded.
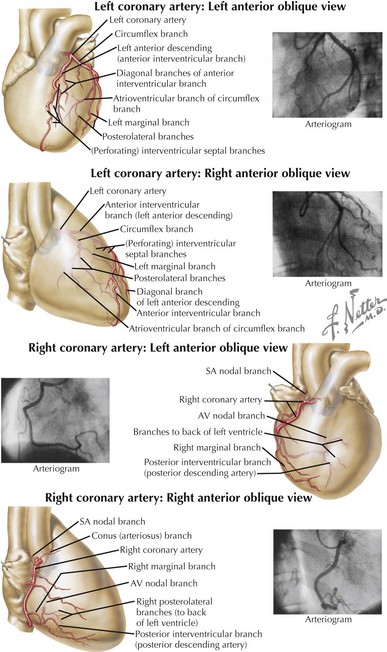
Complete evaluation of coronary arteries involves angiography in multiple projections (Figs. 9-3 and 9-4). This is necessary in order to appreciate the three-dimensional aspects of the coronary arteries with this two-dimensional imaging technique. These views are obtained by rotating the imaging system to different positions around the patient, who lies supine on a radiolucent table. Views from the left or right of the patient can be obtained by varying the degrees of the angle. The imaging system can also be rotated from head (cranial) to toe (caudal) positions. Although almost limitless combinations of potential imaging positions exist, several standard views are utilized that in most cases allow full visualization of the coronary arteries. In all cases, multiple views help to delineate vessel tortuosity and avoid potential misinterpretations as a result of either foreshortening of specific areas or overlapping coronary artery branches.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


