Fig. 5.1
Typical cardiac MRI protocol/sequences for imaging for cardiac sarcoidosis, including: scout images; dark blood; T2 weighted; inversion recovery; cinematic (cine) short axis (SA), horizontal long axis (HLA), and vertical long axis (VLA); three chamber; post-gadolinium intravenous contrast perfusion, axial chest, T1 scout and delayed hyperenhancement in SA, HLA and VLA planes. Post-processing is performed at either the MR console or on an independent workstation
The technique of delayed hyperenhancement (DHE) imaging uses an initial T1 scout sequence for determination of the correct inversion time in order to produce nulling (or dark signal intensity) of the myocardium. The correct inversion time is selected by the MR technologist or physician visually inspecting the T1 scout images; the inversion time is selected that shows uniform dark signal intensity within the myocardium. This inversion time is used for subsequent delayed images, typically acquired at 10–15 min after the intravenous contrast injection for the left ventricle. DHE images are usually acquired in three planes: SA, HLA and VLA. DHE imaging can also be targeted for the right ventricle, typically acquired 8–10 min after the intravenous contrast injection.
Post-processing of Cardiac MRI images, performed either at the MRI console or on an independent workstation, generates quantitative measures including ejection fraction, end diastolic/systolic volumes, stroke volume, cardiac output and myocardial mass [6].
Cardiac MRI exams are performed on either 1.5 or 3.0 Tesla magnetic resonance scanners. A flat set of receiver coils placed on the patient’s chest during the exam contains parallel coils to improve signal-to-noise ratio and decrease exam acquisition time.
Cardiac MRI Imaging Features
Imaging Features and Patterns of Disease
Post-inflammatory Scarring
Cardiac sarcoidosis is characterized by patchy foci of high signal intensity in the myocardium on DHE imaging (Fig. 5.2). Foci of hyperenhancement are often located in basal or subepicardial regions but can be seen throughout the LV or RV myocardium [7]. Single foci of DHE may be subtle (Figs. 5.3 and 5.4), necessitating careful attention to MRI technique and consideration of artifacts.
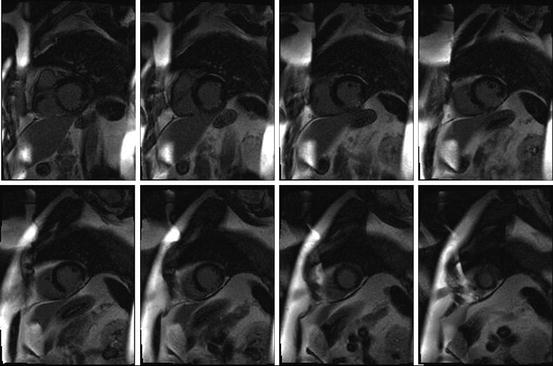
Fig. 5.2
62 year old man with a history of sarcoidosis and non-sustained ventricular tachycardia on Holter monitor. Short axis DHE images show patchy delayed hyperenhancement in the mid inferior and lateral left ventricular walls
Fig. 5.3
48 year old woman with a history of opthalmic sarcoidosis. Chest radiograph and axial post-contrast MRI images show right hilar lymphadenopathy. Short axis and horizontal long axis DHE images show mild patchy delayed hyperenhancement in the inferolateral left ventricular wall and a small pericardial effusion
Fig. 5.4
61 year old woman with a history of sarcoidosis with mediastinal and abdominal lymphadenopathy, inducible ventricular tachycardia/ventricular fibrillation and frequent PVCs. Short axis and horizontal long axis DHE images show mild focal delayed hyperenhancement in the apical lateral wall (arrows). The patient subsequently received an implantable cardioverter defibrillator (ICD)
Acute Inflammation
The inflammatory phase is characterized by focal wall thickening due to infiltration or edema, wall motion abnormalities and high T2 signal intensity [8]. Pathologic features of cardiac sarcoidosis include patchy infiltration of the myocardium in successive stages: edema, non-caseating granulomas, and finally fibrosis or scar [9]. T2 weighted imaging is increasingly being used for tissue characterization in acute myocardial processes.
Wall Motion Abnormality
Three-plane (SA, HLA and VLA) cine imaging is used to assess wall motion. On visual analysis, hypokinetic, akinetic or dyskinetic foci of wall motion abnormality can be secondary to scarred or inflamed myocardium. Navigator tools can be used to confirm wall motion abnormalities in multiple planes.
Associated Features
Depending on the location and extent of cardiac involvement by sarcoidosis, associated features may include ventricular aneurysm or valvular involvement. The pericardium may become thickening and involved by sarcoidosis. Pericardial effusion is not uncommon. Extensive cardiac involvement by sarcoidosis may lead to congestive heart failure. Pulmonary hypertension is common in sarcoidosis (see Chap. 13) with imaging features including central pulmonary enlargement, right heart enlargement and possibly severe pulmonary parenchymal disease including nodularity, architectural distortion and fibrosis.
Differential Diagnosis for Myocardial DHE
Patchy delayed hyperenhancement in the myocardium is not a specific sign for cardiac sarcoidosis. Delayed hyperenhancement can be seen in infarction and other myocardial processes that cause myocardial necrosis, infiltration or fibrosis, including myocarditis, hypertrophic cardiomyopathy, amyloidosis, sarcoidosis and other myocardial conditions [10]. When DHE is in a coronary artery vascular distribution and not mid-myocardial in location, the differential diagnosis includes ischemia/infarct (Fig. 5.5).
Fig. 5.5
57 year old woman with a history of left anterior descending (LAD) coronary artery disease with myocardial infarction. Multiplanar DHE images show delayed hyperenhancement in the LAD vascular territory
Extracardiac Findings of Sarcoidosis
Sarcoidosis can involve multiple anatomic structures typically within the field-of-view of a Cardiac MRI or PET/CT exam, including the pericardium, mediastinal and hilar lymph nodes, axillary lymph nodes, the lungs, upper abdominal lymph nodes, spleen, retroperitoneal lymph nodes and bones. Features of pulmonary sarcoidosis include mediastinal and hilar lymphadenopathy, nodularity, centrilobular nodularity, reticular abnormality, ground glass attenuation, perihilar confluent opacities, architectural distortion and pulmonary fibrosis. [18F]fluorodeoxyglucose (FDG) positron emission tomography (PET) whole body imaging can be used for staging, identification of occult sites of disease and identification of sites suitable for biopsy [11].
Limitations of Cardiac MRI in the Diagnosis of Cardiac Sarcoidosis
Cardiac MRI is not a specific imaging modality for cardiac sarcoidosis and attention to correct MRI protocols and technique as well as artifacts and differential considerations is important. Limitations for Cardiac MRI include the length of the scan for the patient (up to an hour) and the geometry of the MRI scanner. Patients with claustrophobia may not be able to tolerate the exam length or proximity of the circular magnet bore and flat chest coils. Patient size may be an issue as obese patients may not fit into the typical 60 cm magnet bore depending on distribution of body adiposity, although 70 cm MRI scanner bores are increasingly available. Contraindications to an MRI exam include renal impairment (estimated glomerular filtration rate less than 30 mL/kg/min) due to the risk of gadolinium-induced nephrogenic systemic fibrosis. The presence of metallic fragments or any non-MRI-compliant materials within the body including conventional pacemakers are contraindications to MRI.
MR-compatible pacemakers are now available and acceptable cardiac MRI image quality is possible without substantial image degradation due to artifacts (Fig. 5.6). MR-conditional pacemakers may make the benefits of cardiac MRI imaging more available for patients with pacemakers [12], both in the diagnosis and followup of cardiac disease.
Fig. 5.6
37 year old woman with a history of atrial tachycardia ablation. Short axis perfusion and DHE images show MR-compatible pacemaker (Medtronic Advisa MRI SureScan) lead at the RV apex. Note artifact from the pacemaker device in soft tissues of the anterior upper chest wall. Arrow points to the pacemaker lead
PET/CT for the Evaluation of Cardiac Sarcoidosis
PET/CT is used in the evaluation for cardiac sarcoidosis by assessing for hypermetabolic activity within the myocardium, implying inflammation, using a PET protocol designed to suppress normal myocardial glucose uptake.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


