Device Loss during Percutaneous Coronary Intervention: Incidence, Complications, and Retrieval Methods
Emmanouil S. Brilakis
Kirk N. Garratt
Fortunately, the frequency of stent—or other device—loss during cardiac catheterization procedures has significantly declined in recent years, in large part because of improvements in equipment design and the almost universal use of premounted stents. Unfortunately, device loss still occurs, and it can be a harrowing experience, because the operator may not be familiar with retrieval equipment and techniques, exactly because the latter are used so infrequently!
Most of the devices that are lost during percutaneous coronary interventions (PCI) are coronary stents. More rarely, the tip of coronary guidewires or even more rarely angioplasty balloons or the tip of balloon catheters may fracture and embolize distally in the coronary arteries.
The goal of this chapter is to provide information on the mechanisms and risk factors of device loss (mainly stents) and to describe some simple and some more advanced retrieval equipment and techniques. A key concept is that a lost stent may not always need to be retrieved. Deploying or crushing a lost stent may be significantly easier, faster, and safer. Retrieving guidewire and balloon catheter fragments also will be reviewed.
INCIDENCE, MECHANISMS, RISK FACTORS, AND CONSEQUENCES OF STENT LOSS
Incidence and Consequences of Stent Loss
Prior to the development of coronary stents, the incidence of coronary interventional equipment loss was very low and consisted mainly of retained guidewire fragments. In a series of 5,400 consecutive percutaneous transluminal coronary angioplasty (PTCA) procedures in 1987, the reported incidence of inadvertently retained equipment was 0.2% (12 cases) (1).
With the development of coronary stents, the incidence of equipment loss increased, because early delivery systems and strategies resulted in occasional stent loss. Stents were available in the United States for noncoronary applications before they were approved for coronary use; these stents were not premounted onto a delivery balloon catheter and required an operator to compress a stent onto a coronary angioplasty balloon for delivery. Not surprisingly, such
“hand-mounted” stents proved to be subject to greater risk of stent loss than the premounted coronary stent delivery systems that followed. The reported frequency of stent loss varied widely, from 1% to 8%. In an early report from the Mayo Clinic, published in 1993, stent misplacement occurred in 3 of 193 patients (1.6%) (2). Stent retrieval was accomplished in all cases using a variety of techniques (loop snare, biliary forceps, retrieval basket, balloon through stent). In a case series from Spain, published in 1996, Alfonso et al. described stent loss in 17 of 495 (3.4%) consecutive patients using a variety of stent designs (3). The lost stent was successfully retrieved in nine patients but embolized distally in eight patients without any clinical sequelae. In another case series from Germany, published in 1996, Elsner reported stent loss in 6 of 419 consecutive procedures (1.43%) (4). Four of these stents were retrieved using a micro-snare and two embolized peripherally without any sequelae.
“hand-mounted” stents proved to be subject to greater risk of stent loss than the premounted coronary stent delivery systems that followed. The reported frequency of stent loss varied widely, from 1% to 8%. In an early report from the Mayo Clinic, published in 1993, stent misplacement occurred in 3 of 193 patients (1.6%) (2). Stent retrieval was accomplished in all cases using a variety of techniques (loop snare, biliary forceps, retrieval basket, balloon through stent). In a case series from Spain, published in 1996, Alfonso et al. described stent loss in 17 of 495 (3.4%) consecutive patients using a variety of stent designs (3). The lost stent was successfully retrieved in nine patients but embolized distally in eight patients without any clinical sequelae. In another case series from Germany, published in 1996, Elsner reported stent loss in 6 of 419 consecutive procedures (1.43%) (4). Four of these stents were retrieved using a micro-snare and two embolized peripherally without any sequelae.
Stent failure occurred in 108 of 1,303 (8.3%) Canadian patients in whom stenting was attempted between March 1994 and June 1996, as reported by Cantor (5). Out of 134 failed stents, 45% were successfully retrieved, 38% embolized peripherally, 13% were deployed proximal to the target lesion, and 4% remained underdeployed or partially deployed in the left main artery. Urgent CABG was required in 17 (16%) cases.
Finally, in the most recent large series of 2,211 consecutive patients undergoing stent implantation between 1995 and 1999 in Germany, reported by Eggebrecht, intracoronary stent loss occurred in 0.9% (6). Stent loss occurred in 12 of 1,147 manually crimped stents (1.04%) and 8 of 2,919 premounted stents (0.27%, p <0.01). Three of the 20 patients in whom a stent was lost in the coronary circulation underwent emergency coronary artery bypass surgery because of myocardial ischemia, and all three died (6).
In summary, the incidence of stent loss appears to be declining with the use of premounted stents, but may still occur in about 1% of patients. Although stent loss does not seem to carry high risk, it occasionally can lead to serious complications, including emergency coronary artery bypass surgery (6), coronary thrombosis and myocardial infarction (MI) (4,7), cerebrovascular embolic events (if the stent is lost in the ascending aorta), or death (6). Stent loss may identify a population of patients at increased risk for late adverse clinical events, which may or may not be the consequence of the stent loss.
Mechanisms and Risk Factors for Stent Loss
Because stent loss remains an infrequent occurrence, little is understood about the mechanisms and risk factors predisposing to stent loss. Stent loss appears to occur through the following mechanisms (Fig. 42.1):
The stent may be stripped free of its delivery balloon catheter while it is being advanced into a diseased coronary artery segment.
After an unsuccessful attempt to advance a stent through a lesion, the stent may become stuck within the lesion; when the balloon is withdrawn, the stent may come free of the balloon.
If an attempt is made to withdraw a stent back into a guide catheter, the proximal edge of the stent (or, less commonly, a deformed tine of the stent that protrudes away from the balloon catheter) may catch the guide tip, and the stent may be stripped from the balloon once the latter is withdrawn. This appears to be the most common mechanism (6).
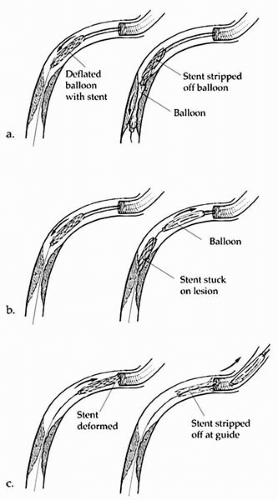 Figure 42.1. Mechanisms that can lead to stent loss: (A) the stent is stripped off the balloon while attempting to cross a tight coronary lesion; (B) after trying to cross a lesion, the stent is partially stuck within the lesion and separates from the balloon when the latter is withdrawn; (C) while attempting to withdraw a deformed stent, a stent tine may “catch” on the guide tip; further attempts to withdraw the stent into the guide lead to stent stripping from the balloon. |
The phrase “Predictions are very hard, especially about the future” is especially true in stent or other device loss during coronary intervention, which occurs very infrequently. Although our ability to predict stent loss is limited, several risk factors for stent loss have been recognized. Those factors are related to the patient, the equipment, or the operator:
Patient-related factors. Arterial tortuosity and calcification may limit the deliverability of a stent to a coronary artery lesion. The tighter the lesion, the more difficult it may be to cross, especially in the presence of calcification. Calcified spicules may catch on the edge of the stent or may cause deformation of the stent, leading to stent loss through any of three aforementioned mechanisms.
Equipment-related factors. Poor guide support may decrease stent deliverability to a coronary lesion; the stent may therefore have to be withdrawn back into the guide, potentially stripping it off the balloon in this process. Also, hand-mounted stents are more likely to be lost compared with premounted stents (6), because the industrial stent crimping process is more reliable than the manual process. Because almost all stents used currently in coronary interventions are premounted, this is rarely a contributing factor, and has probably been one of the main reasons for the decreasing incidence of stent loss.
Operator-related factors. Compared to a strategy of predilatation, direct stenting is related to a higher chance of stent loss. The incidence of stent loss in a series of 250 patients in whom direct stenting was performed was 2% (5 patients) (8). Four of the five lost stents were retrieved; one embolized in a branch of the radial artery and could not be retrieved. Also, the operator’s experience plays a role: If significant resistance is encountered while attempting to withdraw a stent into the guide, then removing the entire system (stent, guide catheter, guidewire) en bloc may be preferable to forceful withdrawal of the stent, which may be stripped off the balloon.
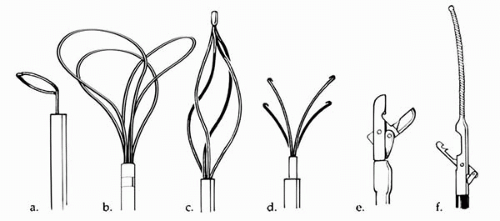 Figure 42.2. Devices useful for recovering damaged stents or other devices lost in the peripheral vasculature. (A) loop snare; (B) En-snare three-loop retrieval system; (C) basket retrieval device; (D) biliary stone forceps; (E) biopsy forceps; (F) Cook retained-fragment retriever. |
RETRIEVAL DEVICES
Several commercially available devices can be used to retrieve lost stents or other equipment (such as wire or balloon fragments) from the coronary arteries and eventually from the body (Fig. 42.2) (2). The availability of retrieval devices varies widely among different laboratories, making it important for every operator be familiar with the locally available devices. Stent loss can be a particularly stressful experience, and some of the stress can be alleviated by prior knowledge of how to use the retrieval devices.
The most commonly used retrieval devices are: (a) the loop snare, (b) the basket retrieval device, (c) the biliary forceps, (d) the biopsy forceps, and (e) the Cook retained-fragment retriever.
Loop Snares
Loop snares are among the most frequently utilized retrieval devices. They consist of a movable wire contained within an outer plastic catheter (Fig. 42.2A). The loops are designed to open at a 90° angle from the delivery catheter, thus facilitating retrieval of the lost devices. The loop is usually made of nitinol, with diameters ranging from 2 to 35 mm; the catheter diameter ranges from 2.3 to 6 Fr, and the length from 48 to 175 mm (Microvena Amplatz GOOSE NECK Snares and Microsnares, ev3 Inc, Plymouth, Minnesota).
A more complex snare configuration is the En Snare retrieval and manipulation system (Medical Device Technologies, Gainesville, Florida), which consists of three interlaced, cabled super-elastic nitinol preformed loops. The multiple loops increase the likelihood of encircling and retrieving the lost device with at least one of the loops (Fig. 42.2B). The snare diameter ranges from 2 to 45 mm, and the length from 120 to 175 mm.
If a commercial loop is not available, a snare can be made in the catheterization laboratory using an exchange
length (300 cm) coronary guidewire and a 5 Fr diagnostic coronary catheter (usually a multipurpose catheter) (Fig. 42.3). The guidewire is inserted into the catheter, and once its end exits from the distal tip of the catheter, it is reinserted until it exits from the proximal end. A disadvantage of homemade snares is that the snare exits at the catheter tip in the direction of the long axis of the catheter and not at a 90° angle, as do the commercial loop snares. Also, some commercial loop snares have a gold coating that greatly enhances their visibility under fluoroscopy.
length (300 cm) coronary guidewire and a 5 Fr diagnostic coronary catheter (usually a multipurpose catheter) (Fig. 42.3). The guidewire is inserted into the catheter, and once its end exits from the distal tip of the catheter, it is reinserted until it exits from the proximal end. A disadvantage of homemade snares is that the snare exits at the catheter tip in the direction of the long axis of the catheter and not at a 90° angle, as do the commercial loop snares. Also, some commercial loop snares have a gold coating that greatly enhances their visibility under fluoroscopy.
Basket Retrieval Device
The basket retrieval device consists of a set of helically arranged loops that can be expanded or collapsed (Fig. 42.2C). Originally designed to remove ureteral and biliary stones, this device can be used to trap lost or retained components within its loops. It can be used to catch a stent from the side and pull it free of a deployment balloon. This device works best if the stent has been damaged and misshapen, so that a portion of the stent projects laterally away from the deployment balloon. Under some circumstances, it may be possible to recover the stent without sacrificing the position of the coronary guidewire across the target lesion. Basket retrieval devices are available commercially from several companies and are available in a variety of expanded sizes and catheter lengths.
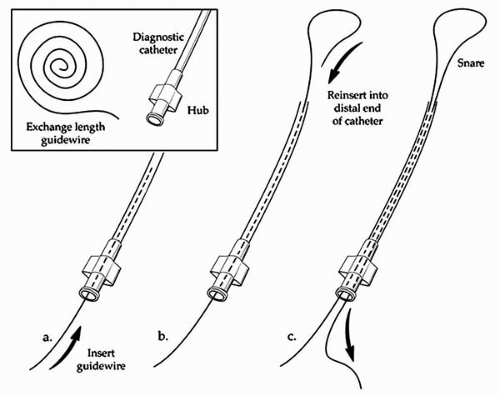 Figure 42.3. How to make a homemade snare: An exchange length (300 cm) coronary guidewire is inserted into a 5 Fr diagnostic coronary catheter (usually a multipurpose catheter) and, once its end exits from the distal tip of the catheter, it is reinserted until it exits from the proximal end of the catheter. |
Biliary Stone Forceps
A biliary stone forceps device consists of a set of curved, fingerlike projections that can be expanded/extended or contracted/retracted (Fig. 42.2D). This device was originally designed for the percutaneous removal of stones from the biliary tree. Manipulating the “fingers” of this device, an operator can snag lost or retained components. This device is most useful in recovering partially expanded stents, or in situations in which a portion of a stent has become separated from the deployment balloon catheter. Under these circumstances, it is often possible to remove a damaged stent without having to lose the guidewire position. Biliary forceps are available with catheter bodies of 4 to 5 Fr, and in lengths of 130 cm. The retracted device has fair visibility under fluoroscopy, but the extended fingerlike projections have poor radio-opacity. The device should be used with great caution in the vascular system because laceration of the vessel wall can occur if the retrieved item becomes entrapped in the fingerlike projections of the device.
Biopsy Forceps
These devices have distal tip modifications that allow grasping of structures through a “biting jaws” action (Fig. 42.2E). Myocardial biotomes are the most familiar example of such a tool. A variety of forceps are available, but most are not available for vascular use because (a) the shaft diameter is very large, (b) the device is too rigid to be passed safely in the arterial system, and /or (c) the catheter length (often 80 to 90 cm) may be inadequate. The thinner, softer, and longer disposable biotomes may be useful in stent retrieval (9). Although biotome jaws are not meant for cutting through metal, it is possible that aggressive gripping with such a device could sever a thin metal stent.
Cook Retained-Fragment Retriever
The Cook retained-fragment retriever catheter, manufactured by Cook, Inc. (Bloomington, Indiana) has a guidewire attached to the distal end, resembling a fixed-wire angioplasty balloon catheter (Fig. 42.2F). An articulating arm operable from the proximal hub permits grasping and retrieving of retained equipment fragments. This catheter was developed for use by vascular radiologists and is available in 80 cm and 145 cm lengths.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


