Dilated cardiomyopathy results from extensively damaged myocardial muscle fibers. This disorder interferes with myocardial metabolism and grossly dilates all four chambers of the heart, giving the heart a globular shape. In this disorder, hypertrophy may be present. Dilated cardiomyopathy leads to intractable heart failure, arrhythmias, and emboli. Because this disease isn’t usually diagnosed until it’s in the advanced stages, the patient’s prognosis typically is poor.
CAUSES AND INCIDENCE
The cause of most cardiomyopathies is unknown. (See Comparing cardiomyopathies, page 68.) Occasionally, dilated cardiomyopathy results from myocardial destruction by toxic, infectious, or metabolic agents, such as certain viruses, endocrine and electrolyte disorders, and nutritional deficiencies.
Other causes include muscle disorders (myasthenia gravis, progressive muscular dystrophy, and myotonic dystrophy), infiltrative disorders (hemochromatosis and amyloidosis), and sarcoidosis. Cardiomyopathy also may be a complication of alcoholism. In such cases, it may improve with abstinence from alcohol but recurs when the patient resumes drinking.
How viruses induce cardiomyopathy is unclear, but researchers suspect a link between viral myocarditis and subsequent dilated cardiomyopathy, especially after infection with poliovirus, coxsackievirus B, influenza virus, or human immunodeficiency virus.
Metabolic cardiomyopathies are related to endocrine and electrolyte disorders and nutritional deficiencies. Thus, dilated cardiomyopathy may develop in patients with hyperthyroidism, pheochromocytoma, beriberi (thiamine deficiency), kwashiorkor (protein deficiency), or eating disorders. Cardiomyopathy may also result from rheumatic fever, especially among children with myocarditis.
Antepartum or postpartum cardiomyopathy may develop during the last trimester or within months after delivery. Its cause is unknown, but usually it occurs in multiparous women older than age 30, particularly those with malnutrition or preeclampsia. In these patients, cardiomegaly and heart failure may reverse with treatment, allowing a subsequent normal pregnancy. If cardiomegaly persists despite treatment, the prognosis is poor.
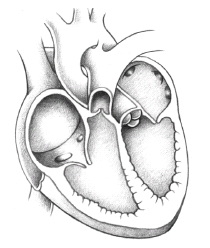
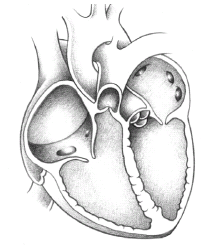
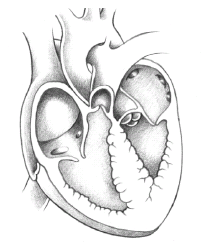
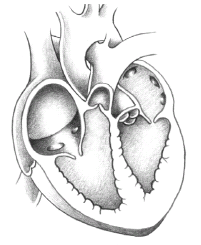
COMPARING CARDIOMYOPATHIES
Cardiomyopathies include various structural or functional abnormalities of the ventricles. They’re grouped into three main pathophysiologic types—dilated, hypertrophic, and restrictive. These conditions may lead to heart failure by impairing myocardial structure and function.
Regardless of the cause, extensive damage to myocardial muscle fibers decreases contractility in the left ventricle. As systolic function declines, stroke volume, ejection fraction, and cardiac output fall. As end-diastolic volumes rise, pulmonary congestion may occur. The elevated end-diastolic volume triggers a compensatory response to preserve stroke volume despite a reduced ejection fraction. Sympathetic nervous system stimulation increases heart rate and contractility. Renal stimulation causes sodium and water retention. And stimulation of the renin-angiotensin-aldosterone system causes vasoconstriction. When these compensatory mechanisms can no longer maintain cardiac output, the heart begins to fail. Left ventricular dilation occurs as venous return and systemic vascular resistance rise. Eventually, the atria also dilate as more work is required to pump blood into the ventricles. Blood pooling in the ventricles increases the risk of emboli.
Dilated cardiomyopathy occurs in 2 of every 100 people and affects all ages and sexes. It’s most common in adult men.
SIGNS AND SYMPTOMS
In dilated cardiomyopathy, the heart ejects blood less efficiently than normal. Consequently, a large volume of blood remains in the left ventricle after systole, causing signs of heart failure—both left-sided (shortness of breath, orthopnea, dyspnea on exertion, paroxysmal nocturnal dyspnea, fatigue, dry cough at night) and right-sided (edema, liver engorgement, jugular vein distention).
Dilated cardiomyopathy also produces peripheral cyanosis and sinus tachycardia or atrial fibrillation at rest in some patients because of low cardiac output.
Auscultation reveals diffuse apical impulses, pansystolic murmur (mitral and tricuspid insufficiency from cardiomegaly and weak papillary muscles), and S3 and S4 gallop rhythms. Renal failure may worsen as decreased cardiac output leads to decreased renal perfusion.
• An electrocardiogram (ECG) and angiography rule out ischemic heart disease; ECG also may show biventricular hypertrophy, sinus tachycardia, atrial enlargement and, in 20% of patients, atrial fibrillation and bundle-branch block.
• Chest X-ray shows cardiomegaly —usually affecting all heart chambers—and may show pulmonary congestion, pleural or pericardial effusion, or pulmonary venous hypertension.
• Chest computed tomography scan or echocardiography identifies left ventricular thrombi, global hypokinesia, and the degree of left ventricular dilation.
• Nuclear heart scans, such as multiple-gated acquisition scanning and ventriculography, show heart enlargement, lung congestion, heart failure, and decreased movement or functioning of the heart.
Only gold members can continue reading. Log In or Register to continue