shift for 33% of luminal enlargement (Fig. 11.1). The vessel expansion ratio was significantly smaller after cutting balloon angioplasty than after conventional angioplasty (1.05 versus 1.22; p <0.05). These findings suggest that the predominant mechanism of dilatation after cutting balloon angioplasty is plaque compression or shift rather than vessel expansion, unlike in conventional angioplasty.
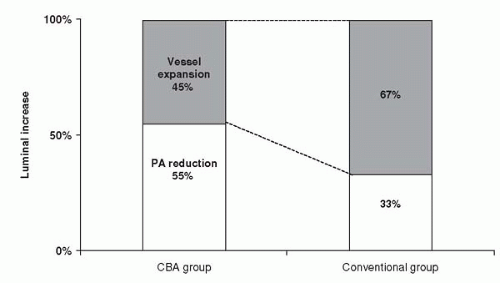 Figure 11.1. Mechanism of luminal increase at the lesion site after cutting balloon angioplasty (CBA) and conventional angioplasty. In the cutting balloon group, plaque area reduction accounted for 55% of the luminal increase and vessel expansion accounted for 45%, whereas the respective values were 33% and 67% in the conventional angioplasty group. |
complex lesions, including ostial and bifurcated lesions. Cutting balloons also are useful as an adjunct to brachytherapy for in-stent restenosis and in bare metal stenting in vessels larger than 3 mm.
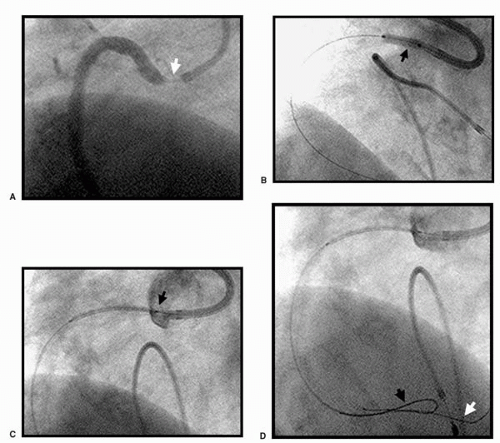 Figure 11.2. (A) Severe high-grade fibrocalcific ostial RCA lesion in an 81-year-old woman (B) Pretreatment with a 3.5 × 10 mm cutting balloon inflated at 8 atm. (C) Placement of the 3.5 × 24 mm Cypher stent, with about 1 mm of the proximal edge of the stent protruding into the aorta, to ensure complete ostial coverage. (D) Buddy wire technique during stent deployment to ensure adequate backup support when the guiding catheter is backed away from the ostium. Black arrow indicates Choice PT Extrasupport wire. White arrow indicates the BMW wire. (E) Postdilatation with a 4.5 × 15 mm Quantum Maverick Balloon at 18 atm and final flaring of the proximal end of the stent in the aorta. (F) Final angiogram showing an acceptable result. (G) Nine-month follow-up angiogram. |
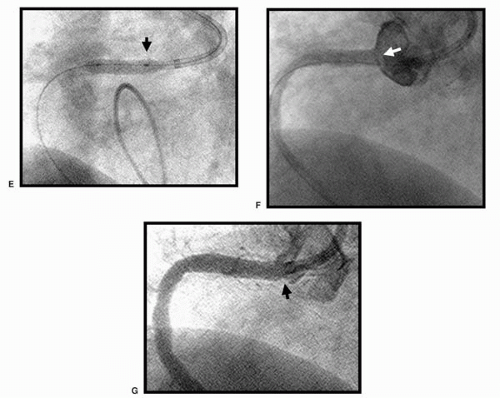 Figure 11.2. (continued) |
registries (54, 55, 56, 57, 58). Direct stenting and conventional BA in bifurcation lesions may cause plaque shifting. The cutting balloon has been demonstrated to minimize plaque shifting (59). Pretreatment using a sequential cutting balloon inflation in bifurcation lesions before stent deployment in the main vessel, followed by final kissing balloon inflation in both vessels, is one possible approach to the management of bifurcation lesion stenting. Provisional stenting of the side-branch vessel is done when suboptimal results are encountered. In short focal lesions, the cutting balloon is only 6 mm in length, thus controlling the injury zone, when compared to predilatation with a conventional balloon.
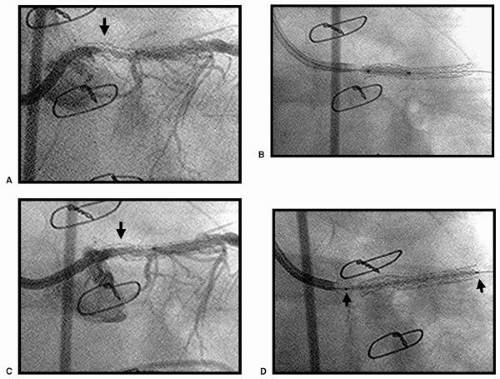 Figure 11.3. (A) High-grade in-stent restenosis of the protected mid left main stem (bare metal stent). (B) Pretreatment with a 3.5 × 10 mm cutting balloon at 6 atm. (C) Angiogram after pretreatment with the cutting balloon. (D) Placement of the 3.5 × 33 mm Cypher Stent extending about 2 mm into the aorta, to ensure full coverage of the ostial left main stem. (E) Postdilatation and flaring of the ostial left main with a 4.5 × 9 mm Quantum Maverick balloon at 18 atm. (F) Final angiographic result. (G) Nine-month follow-up angiogram. |
were randomized, with 153 patients in the cutting balloon group and 153 in the convention angioplasty group (60).
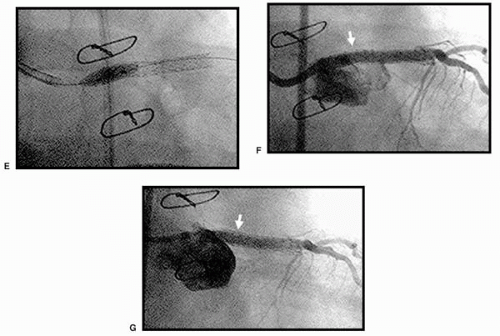 Figure 11.3. (continued) |
TABLE 11.1. CUBA TRIAL | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
randomized to cutting balloon treatment, and 621 to coronary angioplasty. The mean reference vessel diameter was 2.86 ± 0.49 mm, mean lesion length 8.9 ± 4.3 mm, and prevalence of diabetes mellitus in patients was 13%.
TABLE 11.2. CUTTING BALLOON GLOBAL RANDOMIZED TRIAL QUANTITATIVE ANGIOGRAPHIC ANALYSIS | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
angioplasty with conventional BA in small coronary arteries, less than 3 mm in diameter (74).
TABLE 11.3. CBASS TRIAL | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
TABLE 11.4. CAPAS TRIAL
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
|---|