Coronary Blood Flow Measurements
Hajime Sakuma
Charles B. Higgins
Selective coronary angiography has been used to evaluate coronary artery disease. However, an assessment of the anatomic severity of a coronary stenosis does not adequately determine the functional significance of the lesion (1,2). Quantitative coronary angiography, which was designed to minimize variability in interpretation, cannot reliably predict the physiologic significance of a stenosis of intermediate severity (3). An assessment of the functional significance of a stenosis is particularly important in lesions with intermediate severity because the interpretation of such lesions significantly influences therapeutic decisions in patients with coronary artery disease. The functional significance of a coronary arterial stenosis can be evaluated by measuring the coronary flow reserve, which is the ratio of maximal hyperemic coronary flow to the baseline coronary flow (4,5). In the presence of normal epicardial coronary artery and normal myocardial microcirculation, the administration of a vasodilator (e.g., dipyridamole and adenosine) induces approximately a three- to four-fold increase in coronary blood flow. In patients with significant stenoses in the coronary arteries, however, compensatory dilatation takes place in the downstream microcirculation to maintain myocardial blood flow. Thus, the ability to augment coronary blood flow during pharmacologic stress is attenuated in patients with significant coronary arterial stenosis.
The evaluation of blood flow velocity and flow velocity reserve with an intracoronary Doppler guidewire allows a functional assessment of the severity of a stenosis. A study in which an intracoronary Doppler guidewire was used showed that the sensitivity, specificity, and overall predictive accuracy of the coronary flow velocity reserve were 94%, 95%, and 94%, respectively, when stress thallium-201 single-photon emission computed tomography was used as a gold standard (6). Another study demonstrated that a coronary flow velocity reserve below 2 by the Doppler technique had a sensitivity of 92% and specificity of 82% for predicting the presence of a significant stenosis in the coronary artery on selective coronary angiography (7). However, intracoronary flow velocity measurement with a Doppler guidewire is invasive and available only during cardiac catheterization.
Fast phase-contrast cine magnetic resonance imaging (MRI) is an emerging application of MRI that can provide noninvasive assessments of blood flow and flow reserve in human coronary arteries. Several studies have demonstrated the usefulness of this technique in detecting coronary arterial restenosis after percutaneous revascularization procedures and in assessing patency and stenosis in coronary artery bypass conduits. In addition, magnetic resonance (MR) measurement of the coronary sinus blood flow allows the noninvasive assessment of global myocardial blood flow. This chapter reviews the current status and potential clinical applications of MR measurements of blood flow and flow reserve in the coronary artery during coronary artery bypass grafting (CABG).
MAGNETIC RESONANCE IMAGING TECHNIQUES FOR MEASURING CORONARY BLOOD FLOW
Phase-contrast cine MRI can provide noninvasive flow measurements at multiple temporal phases in the cardiac cycle. The MR measurement of blood flow in large vessels—such as the aorta, pulmonary artery, and carotid artery—has been well established and validated (8). However, MR blood flow quantification in the coronary artery has been very challenging because the coronary artery is small (<3 to 4 mm) and subject to both cardiac and respiratory motion. Several different approaches have been proposed in the past for quantifying blood flow in the coronary arteries with MRI, including a time-of-flight method (9), bolus tagging (10), and a phasecontrast method (11). A phase-contrast cine MRI has been most commonly used to measure blood flow in the human coronary vessels in recent studies.
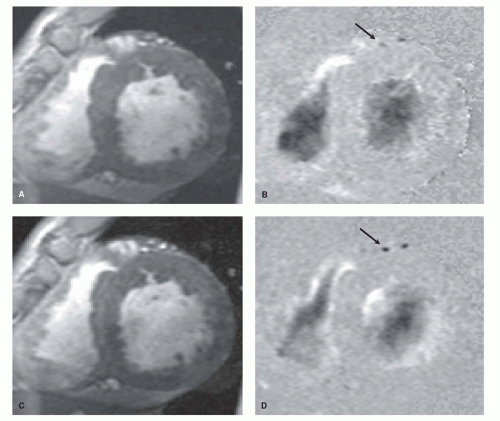 Figure 22.1. Breath-hold phase-contrast cine magnetic resonance (MR) images of the left anterior descending artery (arrows) in a subject without significant stenosis in the left anterior descending artery. Magnitude image (A) and phase-difference image (B) at rest and magnitude image (C) and phase-difference image (D) after intravenous administration of dipyridamole. The increase of the coronary blood flow velocity after pharmacologic stress is observed as a darkening of the signal on phase-difference image. |
MR flow measurement in the coronary artery can be achieved with breath-hold acquisition or respiratory-triggered acquisition. In 1993, Edelman et al. (11) demonstrated the feasibility of breath-hold measurement of blood flow velocity in the coronary artery at a single diastolic phase with the use of a segmented k-space, phase-contrast MR acquisition. Keegan et al. (12) then measured coronary blood flow at multiple phases in the cardiac cycle within a single breathhold time by using segmented k-space, phase-contrast cine MRI. We measured diastolic peak velocities in the left anterior descending artery at rest and during dipyridamole stress with this technique (13). The average coronary flow velocity reserve in eight healthy subjects was 3.14 ± 0.59 (Fig. 22.1). Volumetric blood flow in the coronary arteries can be calculated in theory by integrating the product of the mean velocity and area of the vessel over the cardiac cycle (14,15,16 and 17). The normal coronary flow reserve with volumetric MR flow measurement was 4.2 ± 1.8 according to Grist et al. (16) and 5 ± 2.6 according to Davis et al. (17).
Errors from several sources affect blood flow quantification with phase-contrast MR sequences (18,19 and 20). Currently the major limitations of breath-hold MR measurement of coronary blood flow are suboptimal spatial resolution and temporal resolution. If the spatial resolution of MRI is compromised in relation to the vessel size, partial volume averaging of bright signal from flowing blood and attenuated signal from static tissue around the vessel lumen result in an overestimation of blood flow volume on phase-difference images. In addition, the peak flow velocity in the coronary artery measured by phase-contrast MRI is substantially lower than the peak velocity by intracoronary Doppler guidewire because the highest velocity at the center and lower velocities at the peripheral areas of the vessel lumen are averaged within MRI voxel (21). The lower velocities
that were obtained by phase-contrast MRI, compared with those obtained with intravascular Doppler guidewire, were also observed in CABG (22). Insufficient temporal resolution of the cardiac cycle is another source of the error. If the data acquisition window in the cardiac cycle is insufficient, blurring of the vessel by in-plane motion results in inaccurate measurements of blood flow velocity and flow volume. Hofman et al. (23) reported that the duration of the acquisition window for an accurate MR flow volume quantification should be less than 25 milliseconds for the right coronary artery and 120 milliseconds for the left coronary artery. These figures indicate that further improvement is necessary to obtain accurate flow volume quantification in the right coronary artery. It should be noted that blood flow measured during breath-hold MR acquisition may be different from physiologic blood flow during regular breathing because breath-holding at inspiration causes an increase in intrathoracic pressure, which then reduces systemic venous return to the heart. Our study showed that MR measurements of car diac output are significantly depressed during breath-holding at deep inspiration (24). No significant difference was observed between breath-hold measurement at shallow inspiration and nonbreath-hold measurement, a finding that indicates the importance of using shallow inspiration to obtain physiologic blood flow in breath-hold MR sequences.
that were obtained by phase-contrast MRI, compared with those obtained with intravascular Doppler guidewire, were also observed in CABG (22). Insufficient temporal resolution of the cardiac cycle is another source of the error. If the data acquisition window in the cardiac cycle is insufficient, blurring of the vessel by in-plane motion results in inaccurate measurements of blood flow velocity and flow volume. Hofman et al. (23) reported that the duration of the acquisition window for an accurate MR flow volume quantification should be less than 25 milliseconds for the right coronary artery and 120 milliseconds for the left coronary artery. These figures indicate that further improvement is necessary to obtain accurate flow volume quantification in the right coronary artery. It should be noted that blood flow measured during breath-hold MR acquisition may be different from physiologic blood flow during regular breathing because breath-holding at inspiration causes an increase in intrathoracic pressure, which then reduces systemic venous return to the heart. Our study showed that MR measurements of car diac output are significantly depressed during breath-holding at deep inspiration (24). No significant difference was observed between breath-hold measurement at shallow inspiration and nonbreath-hold measurement, a finding that indicates the importance of using shallow inspiration to obtain physiologic blood flow in breath-hold MR sequences.
Phase-contrast cine MR sequences with respiratorytriggering acquisition permit the nonbreath-hold assessment of coronary blood flow. Navigator techniques are based on one-dimensional image acquisitions; these are used to monitor the position of the diaphragm and accept image data only if the position of the diaphragm is within a certain range. Since image data can be acquired for a prolonged scan time during free breathing, navigator technique makes it possible to acquire phase-contrast cine MR images acquired with better spatial and temporal resolutions. Nagel et al. (25) reported that a higher degree of temporal resolution and shorter acquisition window in the cardiac cycle with navigator-corrected nonbreath-hold MRI increased the accuracy of measurements of coronary blood flow velocity, especially in the right coronary arteries.
The use of fast scan techniques can improve the accuracy of breath-hold MR flow quantification in the coronary vessels (26). In comparison with respiration-triggered acquisition, the breath-hold method requires less scan time; this feature is critically important in studies in which pharmacologic stress is used and makes it possible to assess blood flow and flow reserve in multiple coronary arteries within a short scan time. Langerak et al. (27) used turbo-field echo-planar MRI to measure blood flow in CABG. In this approach, breath-hold flow mapping with spatial and temporal resolutions of 0.8 mm2 and 23 milliseconds, respectively, can be achieved. These investigators showed that breath-hold turbo-field echo-planar MRI provides fast and accurate flow measurements and allows motion-compensated flow quantification in multiple CABGs during a short infusion of adenosine. In a recent study by Keegan et al. (28), high temporal resolution spiral sequences were developed. A free-breathing spiral sequence reduced MRI time by a factor of 10 when compared with a free-breathing FLASH sequence. In addition, a breath-hold spiral sequence can provide an excellent temporal resolution (30 milliseconds) and substantially reduced underestimation of flow velocity that was inevitable with a breath-hold FLASH sequence.
MAGNETIC RESONANCE MEASUREMENT OF CORONARY FLOW RESERVE IN PATIENTS WITH CORONARY ARTERIAL STENOSIS
Measurements of coronary flow reserve obtained with phasecontrast cine MRI can be used to evaluate the functional significance of stenoses in the left main and left anterior descending coronary arteries in patients (Fig. 22.2). To validate this approach, Shibata et al. (21) compared coronary flow velocity reserve measurements obtained by breath-hold phase-contrast cine MRI with measurements by intracoronary Doppler guidewire in 19 patients with varying degrees of stenosis in the left anterior descending arteries. Although the mean MR flow velocity in the coronary artery in the baseline state was significantly lower than that assessed by Doppler guidewire (12.5 ± 4.9 cm/sec vs. 32.4 ± 12.1 cm/sec, p < 0.001), a significant linear correlation was observed between MR and Doppler measurements of the coronary flow velocity reserve, with a correlation coefficient of 0.91. In another study (29), breath-hold MR measurement of the coronary flow velocity reserve in the proximal left anterior descending artery correlated well with myocardial perfusion reserve in the anterior wall of the left ventricle (LV) measured by positron emission tomography (PET) and water labeled with oxygen-15.
The noninvasive MR measurement of coronary flow reserve has been shown to be useful in identifying the functional significance of stenoses in the left anterior descending artery in patients with coronary artery disease. Hundley et al. (30




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
