Despite decades of progress in both prevention and early diagnosis, coronary artery disease (CAD) remains the leading cause of mortality for both men and women in the United States and throughout the Western world (1). For over 40 years, invasive x-ray coronary angiography has been the “gold standard” for the diagnosis of significant (≥50% diameter stenosis) CAD with over a million diagnostic x-ray coronary angiograms performed annually in the United States (1) and higher volumes in Europe and Japan. Although numerous noninvasive tests are available to help discriminate among those with and without significant angiographic disease, studies continue to demonstrate that over 50% of patients referred for elective x-ray coronary angiography are found to have no significant stenoses (2). Despite the absence of disease, these patients remain subjected to the cost, inconvenience, and potential morbidity of invasive x-ray angiography (3,4). In addition, data suggest that in selected high-risk populations, the incidence of subclinical stroke associated with diagnostic cardiac catheterization may exceed 20% (5). Since surgical revascularization of left main (LM) and multivessel proximal coronary disease has the greatest impact on patient mortality, and >90% of coronary segments undergoing intervention fall within the proximal/middle segments (6,7), it would be desirable to have a noninvasive method to directly visualize the proximal/middle native coronary vessels for the accurate identification/exclusion of LM/multivessel CAD.
Over the last decade, coronary magnetic resonance imaging (MRI) has evolved as a potential replacement for diagnostic x-ray coronary angiography among patients with suspected anomalous CAD and coronary artery aneurysms, and has reached sufficient maturity, such that it may obviate the need for invasive x-ray angiography when performed at experienced centers. The technical aspects related to coronary MRI acquisition have been reviewed in a prior chapter.
This chapter will review the published clinical data for coronary MRI in the assessment of anomalous CAD, coronary artery aneurysms, native coronary artery stenoses, and coronary artery bypass graft disease.
Since the mid-1980s, numerous investigators have contributed to our current understanding of the clinical assessment of coronary MRI in comparison with conventional x-ray coronary angiography. The largest body of published clinical experience has used electrocardiogram (ECG)-triggered targeted three-dimensional (3D) segmented k-space gradient-echo and whole-heart steady-state free precession (SSFP) methods, with increasing reports using whole-heart coronary MRI with MR contrast agents and 3-T methods.
MAGNETIC RESONANCE IMAGING OF NORMAL CORONARY ARTERIES
From a historical perspective, conventional ECG-triggered spin-echo MRI was intermittently successful at imaging the native coronary arteries (8,9), but it had relatively low spatial resolution (1.5 × 2 mm). It was the breath-hold, twodimensional (2D) segmented k-space gradient-echo approach described in humans by Edelman (10) that first offered a robust approach for imaging the native coronary arteries. As implemented across numerous vendor platforms, the LM, left anterior descending (LAD), and right coronary artery (RCA) are visualized in the nearly all compliant subjects (Table 21.1) (11,12,13,14,15 and 16). Early reports had reduced (67% to 77%) success for imaging of the left circumflex coronary artery (LCX), a finding likely related to the use of an anterior surface coil (with reduced signal from the posteriorly directed LCX). Improved (>95%) success has been reported with the now routine use of anterior and posterior thoracic phased array cardiac/thoracic coils. Despite relatively limited spatial resolution, normal proximal coronary artery diameter is similar to values obtained by x-ray coronary angiography and pathology (22,23). Currently, both targeted 3D segmented k-space gradient-echo and wholeheart SSFP coronary MRI methods have been the dominant imaging approaches with reported successful visualization of all of the major vessels in nearly every subject (Table 21.1) (21,20). In addition to improved visualization of the origin of the native coronary arteries, another distinct advantage of the 3D approaches is increased contiguous visualization of length/distal segments, as compared with 2D methods. With 3D coronary MRI, similar success (as measured by length of coronary artery seen) is found among healthy adults and patients with angiographic CAD (17,18 and 19,24).
TABLE 21.1 Successful Visualization of the Native Coronary Arteries Using 2D and 3D Segmented 1 k-space Gradient-echo Coronary Magnetic Resonance Imaginga
aIncluding 18 heart transplant recipients. GRE, gradient echo; Resp Comp, respiratory compensation; BH, breath-hold; Sub, subjects; RCA, right coronary artery; LM, left main coronary artery; LAD, left anterior descending coronary artery; LCX, left circumflex coronary artery.
ANOMALOUS CORONARY ARTERY IDENTIFICATION
The ability of coronary MRI to reliably identify the major coronary arteries led to its early adoption for the identification and characterization of anomalous CAD. Though uncommon (<1% of the general population) (25,26) and most often benign, congenital coronary anomalies in which the anomalous segment courses anterior to the aorta and posterior to the pulmonary artery are a well-recognized cause of myocardial ischemia and sudden cardiac death, especially among adolescents and young adults (27). These adverse events commonly occur during or immediately following intense exercise and are thought to be related to compression of the anomalous segment or vessel kinking during periods of high cardiac output, or coexistent eccentric stenoses (27). Projection x-ray coronary angiography had traditionally been the imaging modality for the clinical diagnosis and characterization of these anomalies. However, the presence of an anomalous vessel is sometimes only suspected after the invasive procedure, particularly in a case where there was unsuccessful engagement or visualization of a coronary artery. In addition, the declining routine use of a pulmonary artery catheter during x-ray coronary angiography has made characterization of the anterior versus posterior trajectory of the anomalous vessels more difficult to discern.
Coronary MRI has several advantages in the diagnosis of coronary anomalies. In addition to being noninvasive and not requiring ionizing radiation (an important consideration among this group that is dominated by adolescents and younger adults) or iodinated contrast agents, coronary MRI provides a definitive 3D “road map” of the mediastinal structures. With 3D coronary MRI, one can subsequently acquire and/or reconstruct an image in arbitrary single and double oblique orientations (Fig. 21.1).
Early reports of coronary MRI to visualize anomalous coronary arteries included case report confirmation of x-ray angiographic data. Subsequently, there have been at least six published series (28,29,30,31,32 and 33) of patients who underwent a blinded comparison of coronary MRI data with x-ray angiography (Table 21.2). These early coronary MRI studies often used a 2D breath-hold, ECG-triggered segmented kspace gradient-echo approach (28,29,30,31,32 and 33). These 2D coronary MRI studies have uniformly reported excellent accuracy, including several studies in which coronary MRI was determined to be superior to x-ray angiography (31,32). Most centers now use 3D coronary MRI because of superior reconstruction capabilities with similar excellent results (30) (Table 21.2). As a result, clinical coronary MRI is now the preferred test for young patients in whom anomalous disease is suspected or known anomalous disease needs to be further clarified, or if the patient has another cardiac anomaly associated with coronary anomalies (e.g., tetralogy of Fallot). An important technical aspect of coronary MRI for assessment of suspected anomalous CAD is the reduced spatial requirements. Thus, more rapid coronary MRI acquisitions with lower spatial resolution methods are generally sufficient to define the coronary artery origin and course.
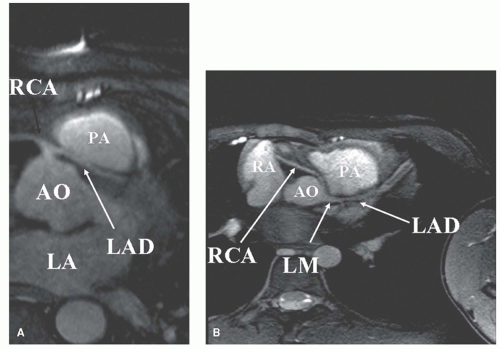
Figure 21.1. Free-breathing 3D coronary MRI using T2 prepulse navigator gating with real-time motion correction. (A) Transverse orientation depicting a malignant-type anomalous LAD originating from the RCA and traversing between the aortic root and the pulmonary artery. (B) Transverse image in another patient with a malignant-type anomalous origin of the RCA from the left coronary cusp. Ao, aorta; PA, pulmonary artery; LA, left atrium; RA, right atrium.
In a somewhat analogous fashion, 2D breath-hold coronary MRI has also been used to define the altered coronary artery orientation in the cardiac transplant population (16). Among cardiac transplant recipients, coronary MRI has documented a 25-degree anterior (clockwise) ostial rotation, likely explaining the more complex coronary engagement during x-ray angiography.
CORONARY ARTERY ANEURYSMS/KAWASAKI DISEASE
Though coronary artery aneurysms are relatively uncommon, data indicate an important role for coronary MRI for assessment of this condition, especially given the common need for serial assessment. The vast majority of acquired coronary aneurysms in children and younger adults are a result of mucocutaneous lymph node syndrome (Kawasaki disease), a generalized vasculitis of unknown etiology, usually occurring in children younger than 5 years. Infants and children with this syndrome may show evidence of myocarditis and/or pericarditis, with nearly 20% developing coronary artery aneurysms. These aneurysms are the source of both short- and long-term morbidity and mortality (46). Approximately half of the children with coronary aneurysms during the acute phase of the disease will have angiographically normal-appearing vessels 1 or 2 years later (46,47). For afflicted young children, transthoracic echocardiography is usually adequate for diagnosing and following these aneurysms, but transthoracic echocardiography is often inadequate after adolescence and in obese children. These patients are therefore often referred for serial x-ray coronary angiographic studies. Data from a series of adolescents and young adults with coronary artery aneurysms (Figs. 21.2 and 21.3) defined on x-ray angiography have confirmed the high accuracy of coronary MRI for both the identification and the characterization (diameter, length) of these aneurysms (Fig. 21.4) (48,49). Though no longitudinal studies have been reported, it is likely that coronary aneurysms can now be effectively followed with serial noncontrast coronary MRI examinations, an approach particularly beneficial for young patients for whom repeated exposure to ionizing radiation is often a concern. Good correlation between coronary MRI and x-ray coronary angiography has also been reported for ectatic coronary arteries (distinct from Kawasaki disease) among adults (50).
TABLE 21.2 Anomalous Coronary Magnetic Resonance Imaging
a Including three patients originally misclassified by x-ray angiography.
b Including five patients unable to be classified by x-ray angiography.
c Including 11 patients unable to be classified by x-ray angiography.
CORONARY MAGNETIC RESONANCE IMAGING FOR IDENTIFICATION OF NATIVE VESSEL CORONARY STENOSES
Although data support a broad clinical role for coronary MRI in the assessment of suspected anomalous CAD and coronary artery bypass graft patency, data are currently in evolution regarding clinical coronary MRI for routine identification of coronary artery stenoses among patients presenting with chest pain under consideration for x-ray angiography, and no efficacy data have been reported regarding “screening coronary” MRI in the general or at-risk populations. However, based on data published from multicenter studies (51,52), for populations in which the concern is LM or multivessel disease coronary MRI approaches are appropriate. More recently, multidetector computed tomography (MDCT) has thrust the noninvasive coronary arterial assessment for CAD in to the limelight with rapid acquisition of high-resolution images of the coronary arteries that has challenged the need for routine coronary x-ray angiography. Coronary MRI has responded to the challenge with further improvements in speed and image quality through advances in hardware, software, and sequence design. Several recent single and multicenter studies using high field strength (3 T), whole-heart acquisitions individually or part of a comprehensive CVMR have shown comparable accuracy to MDCT and single photon emission computed tomography (SPECT) myocardial perfusion imaging (MPI) suggesting more routine use of coronary MRI for the evaluation of CAD may be realized in the near future.
TABLE 21.3 Free-breathing 3D k-space Segmented Gradient-echo Coronary Magnetic Resonance 1 Imaging Using Retrospective and Prospective Navigators for Identification of Focal 1 Greater or Equal to 50% Diameter Coronary Stenoses