Early identification of patients at risk for coronary heart disease is crucial to formulate effective preventive strategies. The elevated risk of coronary artery calcium (CAC) for coronary heart disease is well established. Our aim was to estimate the relative risk of abnormal exercise electrocardiography (Ex ECG) in the presence of CAC. During the year 2001, 566 asymptomatic subjects performed a treadmill exercise test and consented to perform an unenhanced computed tomography to assess CAC. Patients were followed until December 2012. The relative risk for coronary events (acute myocardial infarction, hospitalization for unstable angina or coronary catheterization that resulted in angioplasty or coronary artery bypass surgery), of abnormal Ex ECG and presence of CAC were analyzed. An abnormal Ex ECG was found in 71 subjects (12.5%), and CAC was found in 286 subjects (50.5%). During a mean follow-up of 6.5 ± 3.3 years, 35 subjects experienced a first coronary event. In those without CAC, the rate of coronary events was low (4 of 280; 1.4%) regardless of the Ex ECG results. Subjects with both CAC and abnormal Ex ECG had the highest rate of coronary events (13 of 39; 33%). The adjusted hazard ratio for coronary events, in subjects with CAC, was 5.16 (95% confidence interval 2.52 to 10.60) in those with abnormal Ex ECG compared with those with normal Ex ECG. In conclusion, in subjects with CAC, further risk stratification can be achieved by an Ex ECG, whereas in those without CAC, an Ex ECG has less additional value in predicting coronary events.
Coronary heart disease (CHD) still remains a leading cause of death in the Western world. Approximately 50% of coronary deaths occur in previously asymptomatic subjects. Thus, early and accurate identification of subjects at risk for coronary events is important to institute effective preventive strategies. Conventional risk factors are only partially adequate in achieving this goal as 40% to 70% of patients with myocardial infarction (MI) would not have been recognized as patients at risk using conventional models such as the Framingham score or Prospective Cardiovascular Munster score. Coronary artery calcium (CAC) has been shown to be a sensitive marker of early stages of atherosclerosis. Computed tomography (CT) is an accurate tool for the detection and quantification of CAC and is suggested in the diagnosing of subclinical CHD. The role of an exercise electrocardiogram (Ex ECG) as a screening technique in asymptomatic subjects is controversial. Low exercise capacity and heart rate recovery during exercise tests have been found to predict mortality in several studies. Other studies have demonstrated that ST depression on an Ex ECG does not predict CHD. Currently, exercise testing is not advocated for diagnostic purposes in healthy subjects because of its low specificity and sensitivity. However, exercise tests have been suggested for prognostic use in healthy subjects. The aim of this prospective study was to assess the CHD risk of abnormal Ex ECG in relation with CAC.
Methods
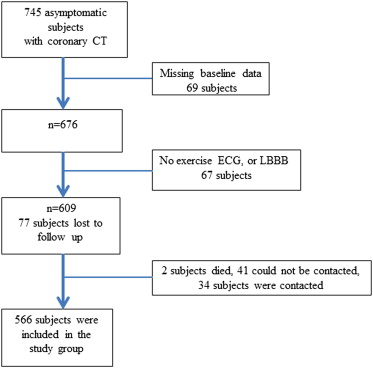
We included subjects examined in our annual check-up clinic between January 2001 and January 2002. Of 1,850 subjects, 745 asymptomatic consecutive subjects who fulfilled the inclusion criteria and consented to perform a screening cardiac CT for CAC evaluation were included. The inclusion criteria were men >40 and women >50 years who were free of CV disease. Of this group, 609 subjects performed a treadmill exercise test and assessment of CAC on the same day. Baseline clinical and laboratory data were also reported. Seventy-seven patients were lost to follow-up, 34 of them were re-contacted and completed telephone questioning regarding coronary events ( Figure 1 ). Thus, 566 asymptomatic subjects constituted our study group. The research protocol was approved by the local institutional review board and complies with the Declaration of Helsinki.
Treadmill exercise testing was conducted in a fasting state using the Bruce protocol. Before stress testing, the 12-channel electrocardiogram at rest was analyzed. According to the protocol, the velocity of the treadmill is accelerated every 3 minutes; the gradient of the treadmill is gradually elevated until the subject reaches his targeted heart rate. The target heart rate was determined according to the following formula: (220 − age). ECG was recorded, and blood pressure (BP) measurements were continued until values returned to baseline levels after discontinuation of the treadmill. Ex ECG was performed with the patient in an upright position. ECG was continuously monitored throughout the test and BP measured every 3 minutes during the load increment stage. Reasons for terminating the exercise was a decrease in BP of 10 mm Hg or more compared with BP at rest, systolic BP >230 mm Hg or diastolic BP >130 mm Hg, horizontal and downsloping ST-segment depressions of >0.3 mV or ST-segment elevations of >0.1 mV, ventricular tachycardia persisting for >30 seconds, an increasing number or polytypic premature beats, disturbed intraventricular or atrioventricular transition, exhaustion of the patient, severe dyspnea, and angina pectoris.
For this study, Ex ECG was considered abnormal when an unequivocal ST depression >0.1 mV (horizontal or downsloping) was recorded during the exercise. Additional non-ST parameters were metabolic equivalents, exercise time, maximal heart rate, and maximal systolic BP. The physician who analyzed the Ex ECG was blinded to the results of the coronary CT.
All CT scans were performed in a single center and analyzed by an experienced physician on a dual-detector spiral CT without ECG gating and without contrast injection; scanning protocol and CAC measuring were implemented according to a previously published protocol using the modified Agatston method. Total CAC score (TCS) was the sum of all the individual calcific lesions identified within the area of the coronary arteries. The reproducibility of calcification scoring by this method is high with intraclass correlation and interobserver agreement coefficients of 0.99 and of 0.94, respectively. A TCS >0 was considered positive for the presence of CAC.
Height and weight were measured with participants wearing light clothing without shoes. Body mass index was calculated as weight (kg)/height (m 2 ). Blood pressure was measured in a seated position after 3 minutes of rest. Hypertension was defined when 2 separate BP readings were ≥140 mm Hg for systolic BP and/or ≥90 mm Hg for diastolic BP, a history of hypertension was reported, or the subject had taken antihypertensive medications.
Diabetes mellitus was defined when fasting plasma glucose was >126 mg/dl (7.0 mmol/L) on 2 separate readings, a history of diabetes mellitus was reported, or the subject had taken insulin or oral hypoglycemic medications. Hypercholesterolemia was defined when measured total cholesterol was >250 mg/dl or when the patient reported taking cholesterol-lowering medications. Smoking status was determined according to the questionnaire; participants were divided into current smokers or nonsmokers.
Estimated glomerular filtration rate (eGFR) was calculated according to the Chronic Kidney Disease Epidemiology Collaboration equation. Framingham score estimating the 10-year cardiovascular risk was calculated for each subject. Subjects were divided into 3 subgroups: <10% (low score), 11% to 20% (moderate score), and >20% (high score).
Subjects’ files were reviewed through 2012. Subjects who were lost to follow-up were contacted, and the coronary end points were assessed by a telephone interview. The end point was delineated as first coronary events, such as acute MI, hospitalization for unstable angina, or coronary catheterization, that resulted in angioplasty or coronary artery bypass surgery.
Data were analyzed by the Statistical Package for the Social Sciences (IBM SPSS Statistics), software version 21.0. Clinical characteristics of study subjects were compared between the following groups: patients with normal and abnormal Ex ECG and according to the presence or absence of CAC. Continuous variables were expressed as mean ± SD. Categorical variables were expressed as frequencies (percentage). Clinical characteristics of study subjects were compared by chi-square tests for categorical variables and independent t tests or analysis of variance tests for continuous variables. Length of follow-up was calculated as time from screening until development of the first coronary event or until the last follow-up date. Incidence of the CHD was analyzed in relation to Ex ECG and the CAC results using the chi-square test with Ex ECG layers. CHD rate was analyzed according to the presence or absence of CAC and normal or abnormal Ex ECG. Hazard ratios (HRs) and 95% confidence intervals (CIs) for incident coronary event by CAC and Ex ECG were estimated by the Cox proportional hazard model adjusting for potential confounders. Conventional risk factors were selected for the model based on previous studies and an association with coronary events in the univariate analysis. Model discrimination was assessed by the C statistics of Harrell et al. The c index is a probability of concordance between predicted and observed survival with c = 0.5 for random predictions and C = 1 for a perfect discriminating model. The c index is relatively unaffected by the amount of censoring. The Kaplan-Meier procedure compared time-to-event models in the presence of censored cases between those with CAC and normal or abnormal Ex ECG. Differences were considered statistically significant at p <0.05.
Results
The study population consisted of 566 subjects (88% men) with a mean age of 55.5 ± 7.3 years. Seventy-one (12.5%) subjects had abnormal Ex ECG. Those with abnormal Ex ECG had similar characteristics as those with a normal Ex ECG ( Table 1 ).
| Variable | Coronary Artery Calcium | ||||||
|---|---|---|---|---|---|---|---|
| No (N = 280) | Yes (N = 286) | ∗ P value | |||||
| Normal Ex ECG (N – 248) | Abnormal Ex ECG (N = 32) | P Value | Normal Ex ECG (N – 247) | Abnormal Ex ECG (N = 39) | P value | ||
| Men | 205 (83%) | 25 (78%) | 0.496 | 232 (94%) | 37 (95%) | 0.887 | <0.001 |
| Age (years) | 53 ± 7 | 53 ± 6 | 0.996 | 58 ± 7 | 59 ± 8 | 0.247 | <0.001 |
| Body Mass Index (Kg/m 2 ) | 27.0 ± 3.5 | 26.1 ± 3.5 | 0.151 | 27.2 ± 3.1 | 27.4 ± 3.8 | 0.635 | 0.351 |
| Systolic blood pressure (mm Hg) | 123 ± 16 | 124 ± 21 | 0.849 | 128 ± 15 | 130 ± 15 | 0.495 | 0.001 |
| Diastolic blood pressure (mm Hg) | 78 ± 9 | 77 ± 10 | 0.561 | 79 ± 9 | 77 ± 6 | 0.124 | 0.309 |
| Heart rate (beats/min) | 79 ± 13 | 78 ± 12 | 0.725 | 76 ± 12 | 77 ± 11 | 0.664 | 0.056 |
| Hypertension | 43 (17%) | 6 (19%) | 0.851 | 80 (33%) | 18 (43%) | 0.096 | <0.001 |
| Diabetes Mellitus | 12 (5%) | 0 (0) | 0.202 | 26 (11%) | 6 (15%) | 0.381 | 0.002 |
| Hypercholesterolemia | 102 (42%) | 10 (31%) | 0.239 | 118 (49%) | 21 (55%) | 0.485 | 0.031 |
| Smoker | 31 (12%) | 4 (12%) | 0.999 | 56 (23%) | 4 (10%) | 0.077 | 0.007 |
| Positive Family history | 57 (23%) | 10 (31%) | 0.321 | 66 (27%) | 9 (24%) | 0.727 | 0.497 |
| Framingham Score (%) | 10.9 ± 3.3 | 10.8 ± 3.4 | 0.950 | 12.5 ± 2.8 | 12.9 ± 2.6 | 0.388 | <0.001 |
| Low score | 198 (80%) | 25 (78%) | 123 (50%) | 17 (44%) | |||
| Intermediate score | 45 (18%) | 5 (16%) | 96 (39%) | 17 (44%) | |||
| High score | 5 (2%) | 2 (6%) | 0.348 | 28 (11%) | 5 (13%) | 0.758 | 0.499 |
| eGFR (ml/min) | 78 ± 13 | 78 ± 11 | 0.986 | 75 ± 12 | 74 ± 12 | 0.633 | 0.002 |
| Serum Glucose (mg/dL) | 97 ± 19 | 92 ± 114 | 0.197 | 104 ± 29 | 102 ± 20 | 0.633 | <0.001 |
| Serum Cholesterol (mg/dL) | 201 ± 34 | 195 ± 28 | 0.389 | 199 ± 34 | 201 ± 31 | 0.720 | 0.731 |
| Serum Triglyceride (mg/dL) | 146 ± 78 | 161 ± 113 | 0.359 | 138 ± 76 | 146 ± 68 | 0.523 | 0.181 |
| Serum HDL Cholesterol (mg/dL) | 45 ± 12 | 49 ± 17 | 0.113 | 44 ± 10 | 44 ± 13 | 0.912 | 0.202 |
| Serum LDL Cholesterol (mg/dL) | 127 ± 28 | 119 ± 27 | 0.164 | 127 ± 30 | 128 ± 28 | 0.947 | 0.590 |
| METS | 12.0 ± 6.3 | 11.8 ± 2.6 | 0.877 | 12.0 ± 6.4 | 11.5 ± 2.1 | 0.627 | 0.309 |
| Exercise time (minutes) | 10.5 ± 6.6 | 10.1 ± 2.9 | 0.873 | 9.9 ± 2.2 | 10.2 ± 2.1 | 0.917 | 0.193 |
| Maximal heart rate (beats/min) | 159 ± 13 | 159 ± 15 | 0.973 | 154 ± 13 | 151 ± 14 | 0.166 | <0.001 |
| Maximal systolic blood pressure (mm Hg) | 175 ± 22 | 176 ± 19 | 0.892 | 189 ± 86 | 179 ± 46 | 0.529 | 0.021 |
| Total calcium score (units) | 0 | 0 | 202 ± 371 | 281 ± 383 | 0.218 | ||
Two hundred and eighty-six (50.5%) subjects had CAC (TCS >0). Subjects with CAC were older (p <0.001) and more likely to be men and smokers; had a higher systolic BP, serum glucose, and Framingham score (p <0.001) and lower eGFR; and were more likely to have hypertension, diabetes mellitus, and hypercholesterolemia than those without CAC ( Table 1 ).
During a follow-up of 11 years (mean 6.5 ± 3.3), 35 subjects experienced a first coronary event, 12 experienced an acute MI, 4 unstable angina pectoris, and 19 subjects underwent coronary catheterization resulting in percutaneous coronary intervention (n = 13) or coronary artery bypass surgery (n = 6).
Subjects who experienced coronary events were older, had a higher Framingham risk score, and were more likely to have hypertension, CAC, and an abnormal Ex ECG than those without events ( Table 2 ). In those with an abnormal Ex ECG, 14 (19.7%) experienced a coronary event; in those with CAC, 31 (11%) experienced a coronary event.
| Variable | Coronary event | ||
|---|---|---|---|
| No (N = 531) | Yes (N = 35) | P value | |
| Men | 465 (88) | 34 (97) | 0.097 |
| Age (years) | 55 ± 7 | 59 ± 8 | 0.002 |
| Body Mass Index (Kg/m 2 ) | 27 ± 3 | 27 ± 3 | 0.904 |
| Systolic blood pressure (mm Hg) | 126 ± 17 | 128 ± 15 | 0.437 |
| Diastolic blood pressure (mm Hg) | 79 ± 9 | 79 ± 8 | 0.794 |
| Heart rate (beats/min) | 78 ± 13 | 72 ± 9 | 0.012 |
| Hypertension | 205 (39%) | 27 (77%) | <0.001 |
| Diabetes Mellitus | 70 (13%) | 5 (14%) | 0.852 |
| Hypercholesterolemia | 233 (45%) | 18 (53%) | 0.367 |
| Smoker | 88 (23%) | 7 (28%) | 0.535 |
| Positive Family history | 133 (25%) | 9 (27%) | 0.804 |
| Framingham Score (%) | 11.6 ± 3.2 | 12.8 ± 2.3 | 0.010 |
| Low score | 347(66%) | 16(46%) | |
| Intermediate score | 144(27%) | 17(49%) | |
| High score | 38 (7%) | 2 (6%) | 0.025 |
| eGFR (ml/min) | 77 ± 13 | 73 ± 10 | 0.057 |
| Serum Glucose (mg/dL) | 100 ± 24 | 98 ± 19 | 0.649 |
| Serum Cholesterol (mg/dL) | 200 ± 33 | 198 ± 34 | 0.717 |
| Serum Triglyceride (mg/dL) | 143 ± 80 | 142 ± 59 | 0.890 |
| Serum HDL Cholesterol (mg/dL) | 45 ± 12 | 43 ± 11 | 0.452 |
| Serum LDL Cholesterol (mg/dL) | 127 ± 29 | 126 ± 31 | 0.855 |
| METS | 11.8 ± 4.6 | 11.2 ± 2.5 | 0.433 |
| Exercise time (minutes) | 10.2 ± 4.8 | 9.6 ± 2.6 | 0.423 |
| Maximal heart rate (beats/min) | 157 ± 14 | 152 ± 11 | 0.083 |
| Maximal systolic blood pressure (mm Hg) | 181 ± 62 | 182 ± 39 | 0.931 |
| Total calcium score (units) | 82 ± 230 | 502 ± 597 | <0.001 |
| Total calcium score >0 | 255 (48%) | 31 (89%) | <0.001 |
| Abnormal exercise ECG | 57 (11) | 14 (40) | <0.001 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


