Fig. 2.1
(a) Circle. The RCA and LCX make a circle along the both atrioventricular grooves. (b) Loop. The LAD and PDA make a loop along the anterior and posterior interventricular grooves
2.2 Dominance
PDA and PL branches supplying inferior wall of left ventricle determine dominance.
Right dominance (85 %): PDA and PL from RCA (Fig. 2.2a).
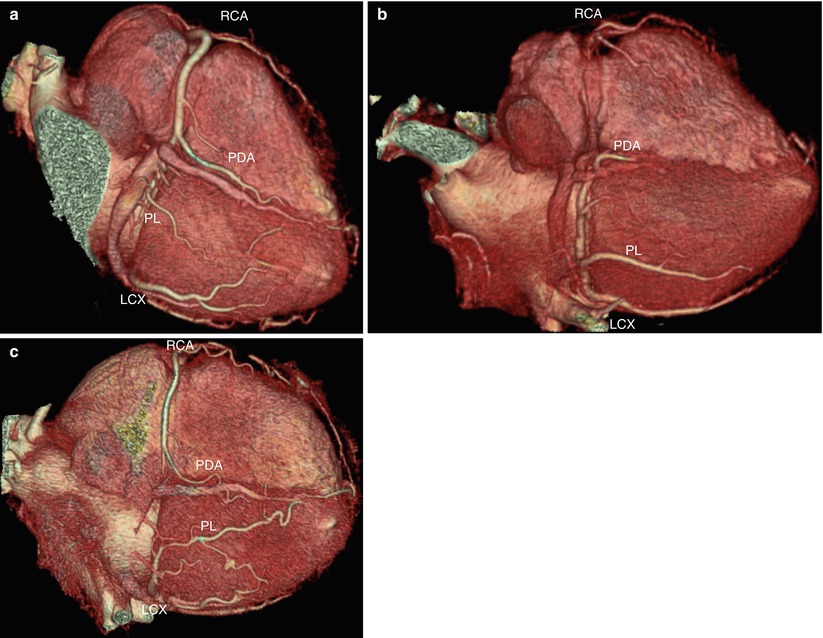
Fig. 2.2
(a) Right dominant supply. The PDA and PL branches arise from the RCA. (b) Left dominant supply. The PDA and PL branches arise from LCX. (c) Codominant supply. PDA arises from the RCA and PL arise from the LCX
Left dominance (8 %): PDA and PL from LCX (Fig. 2.2b).
Codominance (7 %): PDA from RCA and PL from LCX or parallel branch from the right and left coronary arteries (Fig. 2.2c).
2.3 Coronary Arteries
2.3.1 Left Main Coronary Artery
Left main coronary artery usually bifurcates into left anterior descending artery (LAD) and left circumflex artery (LCX) with 5 – 10 mm length and 4 – 5 mm in diameter. Sometimes, it trifurcates into LAD, LCX, and ramus intermedius.
2.3.2 Left Anterior Descending Artery (LAD) (Fig. 2.3a, b)
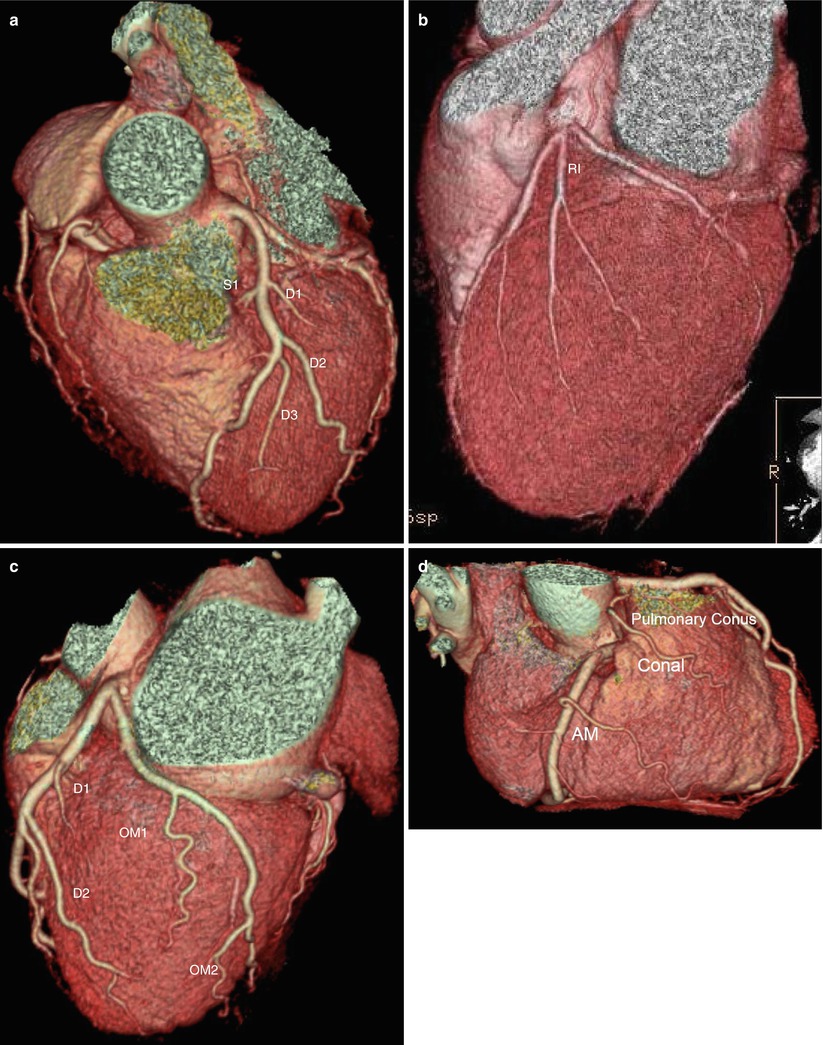
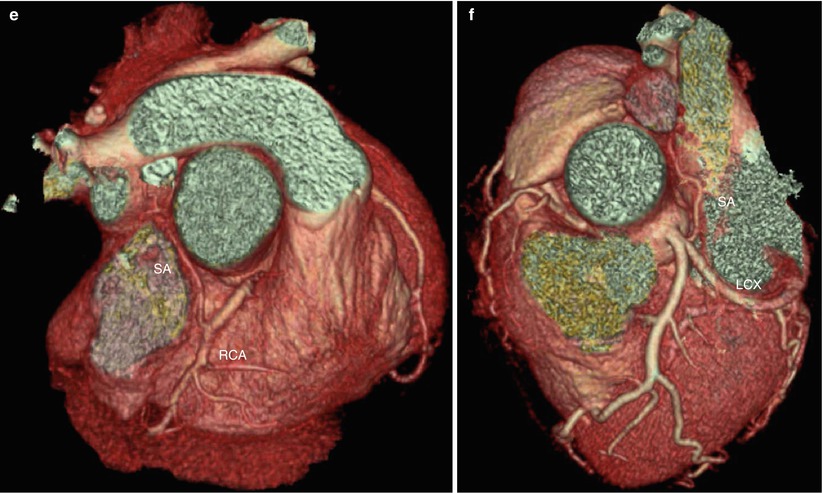
Fig. 2.3
(a) LAD and branches. The first diagonal branch (D1) is close to the first septal branch (S1), and the following second and third diagonal branches (D2 and D3) are well delineated along the free wall of the left ventricle. (b) Ramus intermedius (RI) arises between LAD and LCX orifice. (c) LCX and branches. First and second obtuse marginal branches (OM1, OM2) of LCX supply the lateral portion of LV (obtuse margin). (d) RCA and branches. Conal branch arises from the RCA near the aorta and runs anteriorly to the pulmonary conus. Acute marginal branch (AM) runs along the anterior wall of the right ventricle toward the acute margin. (e, f) Origin of sinonodal artery (SA). SA is originated from the RCA (60 %) or LCX (40 %) and runs to the SVC
Diagonal branches supply the anterolateral wall of the left ventricle. The first branch is usually the largest. These branches are numbered as they arise from the LAD territory such as first diagonal (D1), second diagonal (D2), etc.
Septal branches: perpendicular into the interventricular septum. The first branch is the largest and supplies the His bundle and proximal left bundle branch. It usually originates just beyond the orifice of the first diagonal branch.
Ramus intermedius: originated from LM between LAD and LCX; its course is similar to that of D1.
Proximal LAD: from the orifice to the origin of the first septal branch.
Middle LAD: from the origin of the first septal branch halfway to the apex.
Distal LAD: remained halfway to the apex.
2.3.3 Left Circumflex Artery (LCX) (Fig. 2.3c)
The obtuse marginal branches supply the lateral portion of the left ventricle, numbered as they arise from the LCX such as the first obtuse marginal (OM1), second obtuse marginal (OM2), etc.
Proximal LCX: from the orifice to the large first OM.
Distal LCX: distal to the first OM.
2.3.4 Right Coronary Artery (RCA) (Fig. 2.3d, e)
Conus branch: first branch, very proximally located, supplies the pulmonary conus of the right ventricle (RV). Separate takeoff from aorta is common.
Sinus node artery: 60 % in RCA and 40 % in LCX.
Acute marginal branch: anterior free wall of the RV.
The PDA and PL branches supply the inferior wall of the left ventricle and AV node.
Proximal LAD: from the orifice halfway to acute margin.
Middle LAD: remained halfway to acute margin.
Distal LAD: from acute margin to base of the heart.
2.4 Angiography Versus CT
2.4.1 Basic Angiographic View of the Left Coronary Artery
Right anterior oblique (RAO) caudal: right side of the heart, good view of LCX, OM, and proximal LAD (Fig. 2.4a)

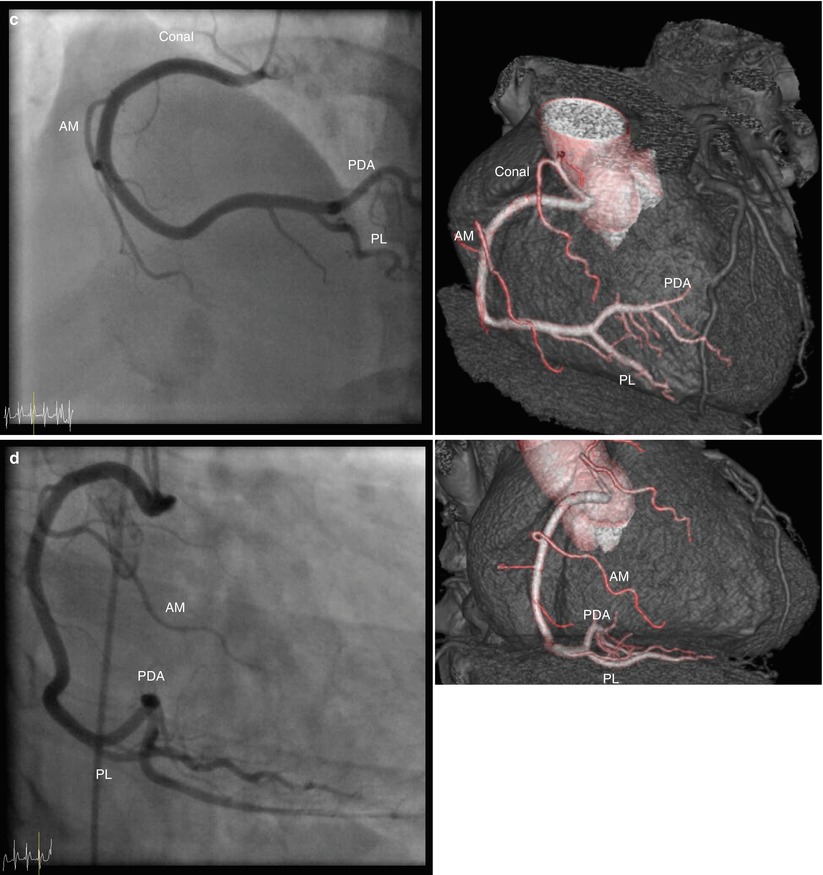
Fig. 2.4
(a) RAO caudal view of the left coronary artery. Angiography and transparent volume rendering image show good view of LCX with obtuse marginal branches (OM1 and OM2) and proximal LAD. (b) LAO caudal view of the left coronary artery. Angiography and transparent volume rendering image show good view of the left main coronary artery, and this view has good delineation of diagonal and septal branches. (c) LAO cranial view of right coronary artery. Angiography and transparent volume rendering image show good view of ostial and proximal RCA. (d) RAO straight view of right coronary artery. Angiography and transparent volume rendering image show good view of middle RCA PDA, posterior descending artery, PL, posterolateral branch, AM, acute marginal branch
2.5 Coronary Artery Variation and Anomalies
2.5.1 Incidence
2.5.2 Clinical Significance
Most anomalies do not create clinical problems.
19–33 % of sudden cardiac deaths in the young population are related to coronary artery anomalies.
Benign (80 %) and potentially serious anomalies (20 %).
2.6 Anomalies of Origin and Course
2.6.1 Anomalous Origin of the Left Coronary Artery from the Pulmonary Artery (ALCAPA) Syndrome (Fig. 2.5)
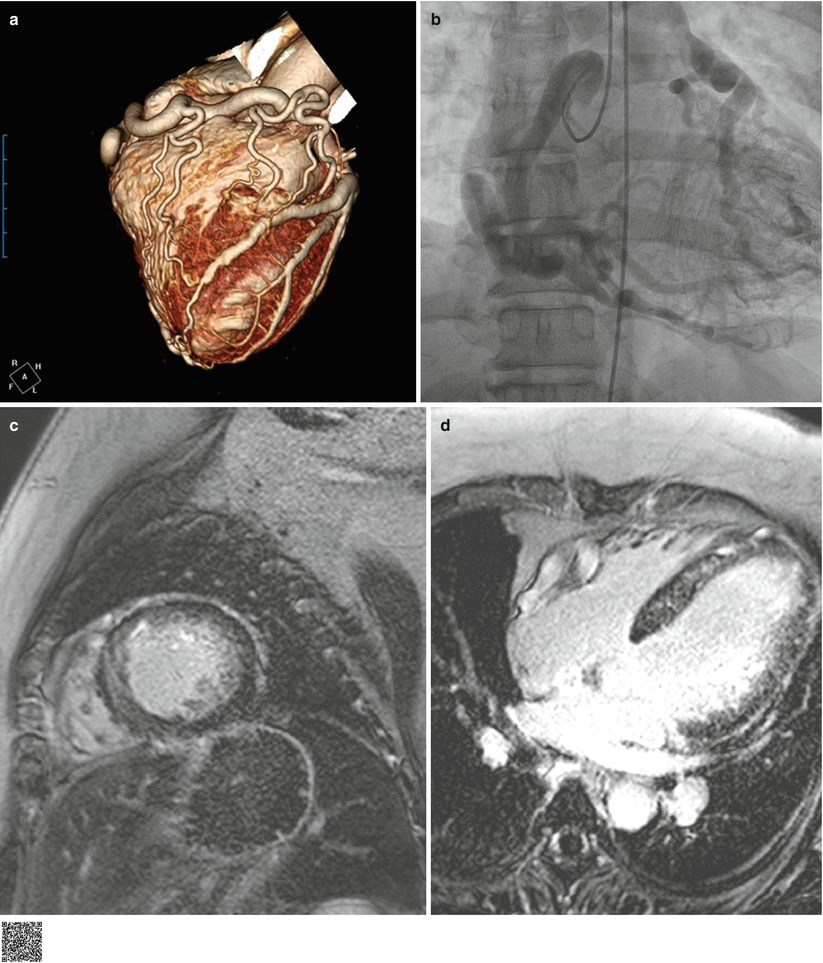
Fig. 2.5
ALCAPA. Right coronary angiography (a) and coronary CTA (b) image show well-developed collaterals from the markedly dilated right coronary artery (RCA) to the dilated and tortuous left coronary artery (LCA) originated from the main pulmonary artery (PA). Delayed enhancement MR (c, d) shows diffuse subendocardial enhancement of the left ventricle, representing diffuse ischemia (http://extras.springer.com/2015/978-3-642-36396-2)
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


