2
Conduction and its problems
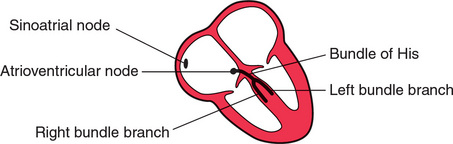
We have already seen that electrical depolarization normally begins in the sinoatrial (SA) node, and that a wave of depolarization spreads outwards through the atrial muscle to the atrioventricular (AV) node, and thence down the His bundle and its branches to the ventricles. The conduction of this wave front can be delayed or blocked at any point. However, conduction problems are simple to analyse, provided you keep the wiring diagram of the heart constantly in mind ( Fig. 2.1).
CONDUCTION PROBLEMS IN THE AV NODE AND HIS BUNDLE
The time taken for the spread of depolarization from the SA node to the ventricular muscle is shown by the PR interval (see Ch. 1), and is not normally greater than 220 ms (six small squares).
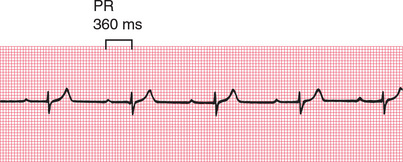
FIRST DEGREE HEART BLOCK
If each wave of depolarization that originates in the SA node is conducted to the ventricles, but there is delay somewhere along the conduction pathway, then the PR interval is prolonged. This is called ‘first degree heart block’ ( Fig. 2.2).
SECOND DEGREE HEART BLOCK
Sometimes excitation completely fails to pass through the AV node or the bundle of His. When this occurs intermittently, ‘second degree heart block’ is said to exist. There are three variations of this:
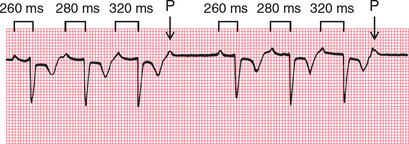
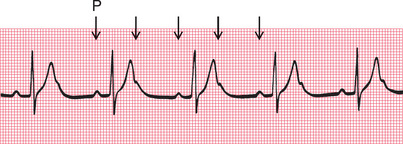
1. There may be progressive lengthening of the PR interval and then failure of conduction of an atrial beat, followed by a conducted beat with a shorter PR interval and then a repetition of this cycle. This is the ‘Wenckebach’ or ‘Mobitz type 1’ phenomenon ( Fig. 2.3).
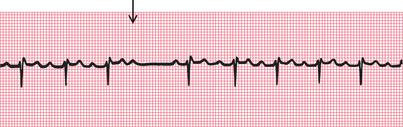
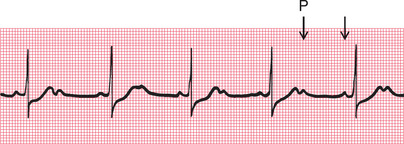
2. Most beats are conducted with a constant PR interval, but occasionally there is atrial depolarization without a subsequent ventricular depolarization. This is called the ‘Mobitz type 2’ phenomenon ( Fig. 2.4).
3. There may be alternate conducted and nonconducted atrial beats (or one conducted atrial beat and then two or three nonconducted beats), giving twice (or three or four times) as many P waves as QRS complexes. This is called ‘2:1’ (‘two to one’), ‘3:1’ (‘three to one’) or ‘4:1’ (‘four to one’) conduction ( Fig. 2.5).
It is important to remember that, as with any other rhythm, a P wave may only show itself as a distortion of a T wave ( Fig. 2.6).
The underlying causes of second degree heart block are the same as those of first degree block. The Wenckebach phenomenon is usually benign, but Mobitz type 2 block and 2:1, 3:1 or 4:1 block may herald ‘complete,’ or ‘third degree’, heart block.
THIRD DEGREE HEART BLOCK
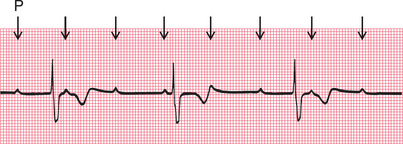
Complete heart block (third degree block) is said to occur when atrial contraction is normal but no beats are conducted to the ventricles ( Fig. 2.7). When this occurs the ventricles are excited by a slow ‘escape mechanism’ (see Ch. 3), from a depolarizing focus within the ventricular muscle.
Complete block is not always immediately obvious in a 12-lead ECG, where there may be only a few QRS complexes per lead (e.g. see Fig. 2.8). You have to look at the PR interval in all the leads to see that there is no consistency.
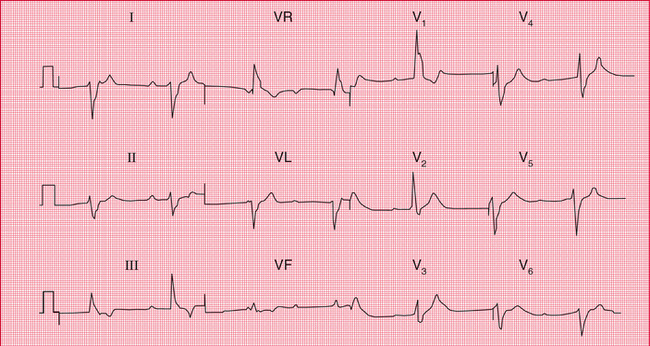
Fig. 2.8 Complete heart block
Note
• Sinus rhythm, but no P waves are conducted
• Broad QRS complexes (duration 160 ms)
• Right bundle branch block pattern
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


