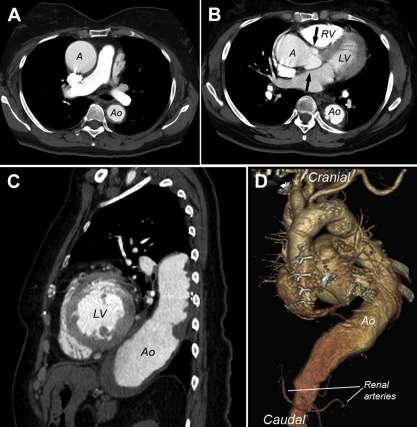
This report describes certain computed tomographic and morphologic features of syphilitic aortitis in 2 patients in whom the process involved the entire thoracic aorta.
In 2009, a report from this institution described certain necropsy features in 90 unoperated patients seen in a 25-year period with syphilis involving the aorta. That report was the first to analyze characteristic features of vascular syphilis since 1964. During a recent 4-month period, we studied at necropsy 2 additional patients with this condition, and the findings in them were unusual enough, in our view, to prompt this report.
Description of Patients
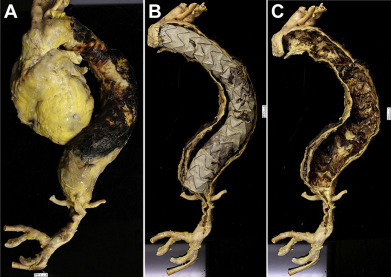
Certain findings in each of the 2 patients are summarized in Table 1 and illustrated in Figures 1 to 3 . Patient #1 had her aneurysmal ascending aorta resected and the aortic valve replaced (bi-leaflet mechanical valve-Carbomedics) at age 68. During the next 10 years, the descending thoracic aorta progressively enlarged. Seventeen days before death, a 36-cm-long stent was placed in the descending thoracic aorta. Postoperatively, movement in the legs progressively decreased and cardiac arrest occurred. The mechanical valve in the aortic-valve position appeared to have functioned properly (This patient was on warfarin chronically.). At necropsy, nearly 2,000 ml of blood was found in the right pleural space, and a rupture site was seen at the bend in the thoracic aorta.
| Variable | Patient | |
|---|---|---|
| #1 | #2 | |
| Age (years) | 78 | 71 |
| Gender | Female | Male |
| Race | Black | White |
| Highest blood pressure (mm Hg) | 180/90 | 145/80 |
| Hypertension (history) | + | + |
| Aortic regurgitation | + | o |
| Obesity | + | + |
| Heart weight (g) | 565 | 410 |
| Operation, aorta | + | o |
| Stent, aorta | + | o |
| Cause of death | Rupture, DTA | Rupture, AAA |
| Cardiac adiposity ∗ | + | + |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


