Internationally, community-acquired pneumonia is a common problem both for community and hospital physicians. It occurs with an annual incidence of about 5-11 per 1,000 adult population and rises with age, to about 34 per 1,000 population for patients aged over 75 years. The annual incidence of patients that require hospital admission varies from approximately 1-4 per 1,000 population. The mortality rates are low (<1%) for patients managed in the community, higher in patients admitted to hospital, around 5-12%, and highest for patients requiring mechanical ventilation with rates from around 35% to >50%. It is thus a common disease and can have considerable impact on health care resources. This section on community-acquired pneumonia, with illustrative radiology, microbiology, and pathology, discusses the investigation, diagnosis, and management of communityacquired pneumonia in adults. Key areas covered include the common causative organisms, patient presentation including severity assessment, a recommended investigation strategy, and treatment options. Finally, the complications of community-acquired pneumonia are illustrated with particular emphasis on the investigation, diagnosis, and management of lung abscess and pleural infection.
Aetiology
In most cases of mild community-acquired pneumonia, a microbiological cause is not determined. When sputum samples are cultured by routine bacteriological methods, the commonest pathogen isolated is Streptococcus pneumoniae. Less commonly, Haemophilus influenzae or Moraxella catarrhalis may be cultured, particularly in patients with previous airways damage.
Some important respiratory pathogens cannot be cultured by routine methods, but are usually detected by immunological or molecular methods. These, the so-called ‘atypical’ causes of pneumonia, include Mycoplasma pneumoniae, Legionella pneumophila, Chlamydia pneumoniae, Chlamydia psittaci, Coxiella burnetti, and respiratory viruses such as influenza viruses, adenoviruses, and respiratory syncytial virus.
Most organisms associated with mild pneumonia can also cause severe community-acquired pneumonia. Particularly severe pneumonia with septic shock may result when viral infections, such as influenza, lead to secondary lung infections with virulent pathogens such as Streptococcus pneumoniae, Staphylococcus aureus, or Streptococcus pyogenes.
Presentation
Patients may have had preceding viral upper respiratory tract symptoms.
New onset of lower respiratory tract symptoms occurs (usually cough ± sputum production [sometimes haemoptysis], breathlessness, fever, and sometimes pleurisy).
Systemic features are often present (general malaise, anorexia, sweating, fevers, shivers, or aches and pains).
Extrapulmonary symptoms can be present.
New onset confusion can arise in severe cases.
New focal chest signs occur. The clinical signs in practice can be highly variable (the classical teaching in lobar pneumonia is reduced expansion, coarse inspiratory crackles, reduced percussion, bronchial breathing, and increased vocal resonance in the affected lobe).
New chest radiographic consolidation is present.
There is no other explanation for illness.
Overall, the likely aetiological agent cannot be accurately predicted from clinical features.
Severity score
To guide placement and treatment, it is helpful to stratify patients according to illness severity. Patients with severe pneumonia have two or more of the following:
New onset mental confusion.
Blood urea >7 mmol/l.
Respiratory rate ≥30/min.
Systolic blood pressure <90 mmHg or diastolic ≤60 mmHg.
Physical findings including respiratory rate ≥30/min, pulse ≥125/min, low blood pressure (systolic <90 mmHg and/or diastolic ≤60 mmHg), and temperature <35°C or ≥40°C.
Laboratory findings with blood urea >7 mmol/l, white blood cell count <4 × 109/l or >20 × 109/l or an absolute neutrophil count <1 × 109/l, and hypoxaemia. The British Thoracic Society guidelines on pneumonia define hypoxaemia as SaO2 <92% or PaO2 <8 kPa (60 mmHg) regardless of inspired oxygen concentration, whereas the American Thoracic Society guidelines on pneumonia define it as PaO2 / FiO2 <250.
Bilateral or multi-lobe involvement of the chest radiograph.
Mycoplasma pneumoniae, Chlamydia pneumoniae, viral infections, e.g. adenovirus
Investigations
The following investigations are routine:
Chest radiograph.
Full blood count.
Urea, electrolytes, and liver function tests.
Inflammatory markers such as erythrocyte sedimentation rate and C reactive protein.
Oxygen saturations on air and arterial blood gases if <92% or in patients with severe pneumonia.
Common chest radiographic abnormalities are presented in Table 1.1.
Overall there are no characteristic features on the chest radiograph that allow the accurate prediction of the likely pathogen. This is normally identified with further microbiological investigations.
Table 1.2 presents the common blood test abnormalities.
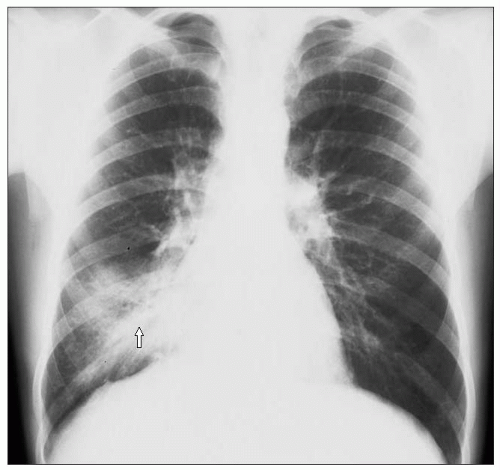
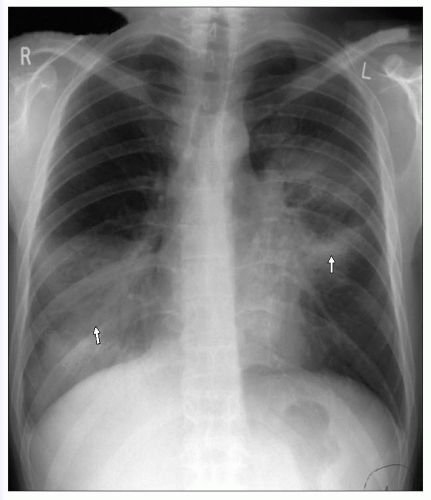
The chest radiograph from a 20-year-old male is shown in 1.1. He presented with a right middle lobe pneumonia due to Streptococcus pneumoniae. Due to consolidation, there is loss of the right heart border in keeping with pneumonia affecting the right middle lobe. The consolidation is limited to the right middle lobe in keeping with a lobar pneumonia.
1.1 Chest radiograph showing right middle lobe consolidation due to lobar pneumonia (arrow).
Table 1.2 Common blood test abnormalities
Test
Abnormalities identified
Full blood count
1 Raised white cell count >10 × 109/l
2 White cell count <4 × 109/l or >20 × 109/l in severe pneumonia
3 Lymphopenia may be present in Legionella and viral pneumonia
4 Normocytic anaemia commonly seen in severe pneumonia
Urea and electrolytes
1 Pre-renal or acute renal failure can develop (increased blood urea >7 mmol/l is an indicator of severe pneumonia)
2 Low sodium can be found due to the syndrome of inappropriate antidiuretic hormone secretion
3 Low albumin
4 Deranged liver function tests often identified; can be related to the pneumonia itself or the antibiotics prescribed
Inflammatory markers
1 Raised erythrocyte sedimentation rate
2 Raised C-reactive protein
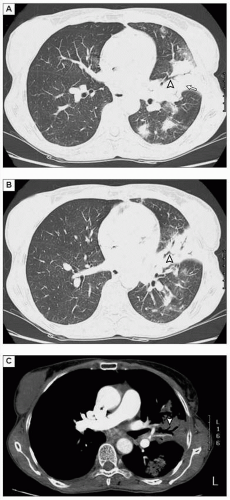
The CT images in 1.2 reveal the features of pneumonia, with air space consolidation and an air bronchogram present. The air bronchogram is seen because patent bronchi are visible against airless alveoli filled with exudative fluid.
1.2A-CCT scans demonstrate pneumonia, with air space consolidation (arrow) and an air bronchogram (arrowhead). (A, B: lung window settings; C: mediastinal window setting.)
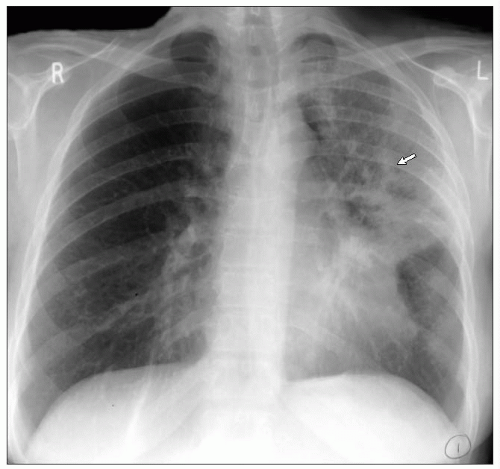
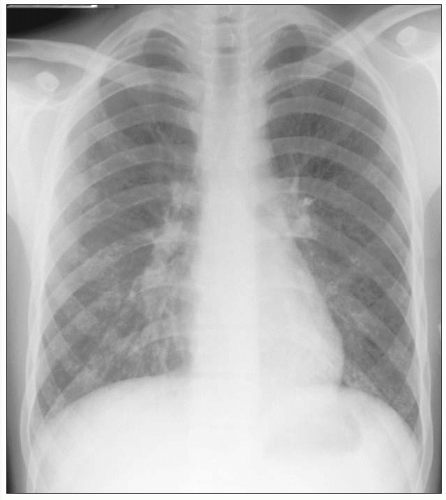
A 57-year-old female presented with left upper lobe pneumonia. No pathogen was isolated but the pneumonia resolved with a 7-day course of amoxicillin and clarithromycin. The chest radiograph is shown in 1.3. There is extensive consolidation with air bronchograms present within the left upper lobe. The consolidation is limited to the left upper lobe in keeping with a lobar pneumonia.
1.3 Chest radiograph showing left upper lobe pneumonia with extensive consolidation and air bronchograms present within the left upper lobe (arrow).
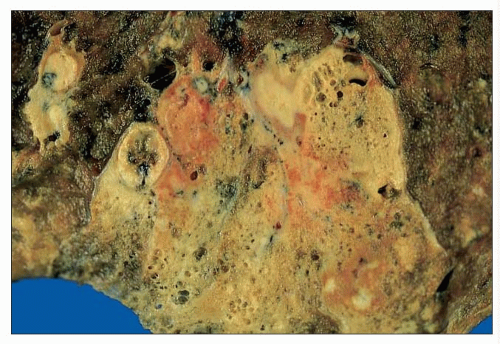
1.4 Macroscopic picture of lung tissue with areas of consolidation and abscess formation within the consolidated lung, due to Staphylococcus aureus infection.
1.4 shows a macroscopic picture of a lung, demonstrating a wedge-shaped area of yellow consolidation which is bounded by fibrous septa. Areas of cavitation and abscess formation can be seen focally within the consolidated lung. The organism responsible in this case was Staphylococcus aureus.
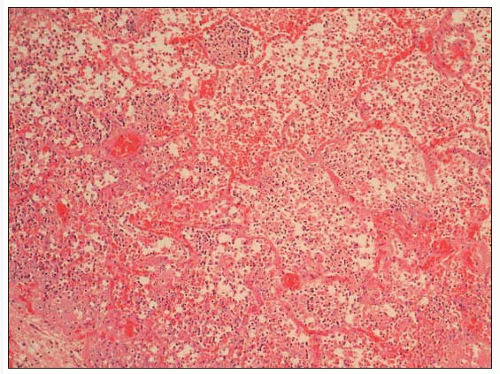
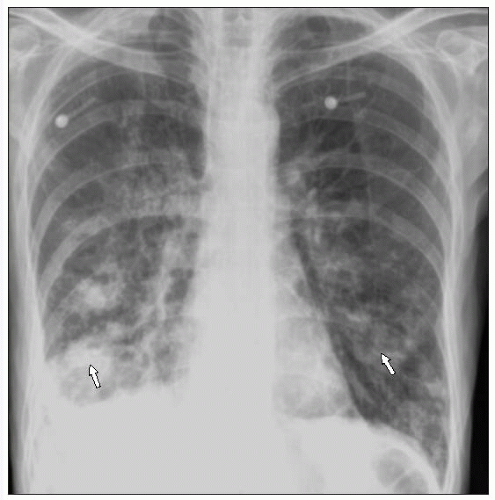
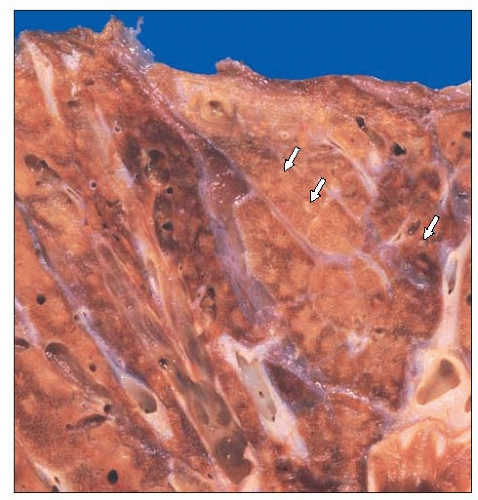
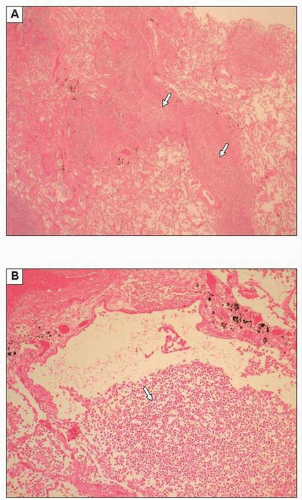
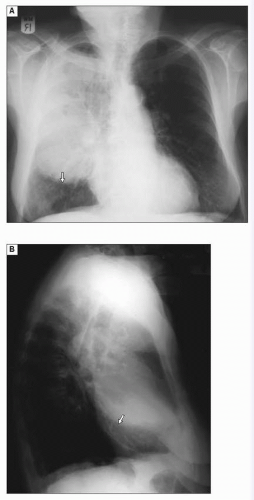
Microscopy from a case of lobar pneumonia is shown in 1.5. The alveolar spaces are filled with neutrophils and fibrin leading to ‘consolidation’ of the lung. In the event of resolution, this inflammatory process is removed and the lung architecture may be left intact. With some organisms, such as Staphylococcus aureus, there may be extensive necrosis and destruction of alveolar walls with healing by scarring. A 66-year-old male presented with severe bilateral bronchopneumonia. The chest radiograph (1.6) demonstrates that there is also a small right pleural effusion and evidence of an old healed right 8th posterior rib fracture. There is patchy bilateral consolidation affecting multiple lobes, in keeping with a bilateral bronchopneumonia. 1.7 presents a macroscopic picture from a case of bronchopneumonia. Unlike in lobar pneumonia, the majority of the lung parenchyma appears normal but spotty areas of pale consolidation are seen. The reason for the focal nature of the change is that the consolidation is centred on the airways rather than diffusely involving the alveolated lung parenchyma. Histologically focal areas of acute inflammation are present in the lung (1.8A, B) which are centred on the airways, with some spilling of inflammatory debris into adjacent alveolar airspaces.
1.5 Microscopy of lung tissue from a case of lobar pneumonia. The alveolar spaces are filled with neutrophils and fibrin leading to ‘consolidation’ of the lung.
1.6 Chest radiograph showing bilateral bronchopneumonia (two areas of consolidation are arrowed). (Courtesy of Dr. T. Sethi, Consultant Respiratory Physician, Royal Infirmary, Edinburgh, Scotland.)
1.7 Macroscopic picture of lung tissue showing focal pale consolidation due to bronchopneumonia (arrows).
1.8A, B Photomicrographs (A: low power; B: high power) of lung tissue from a patient with bronchopneumonia, showing acute inflammatory cells and debris within a bronchus (arrows).
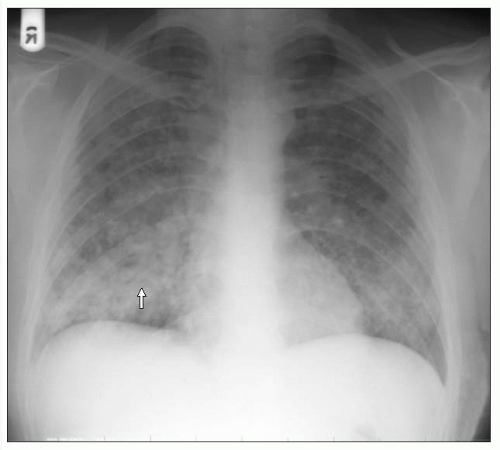
A 37-year-old male presented with a bilateral pneumonia due to Legionella pneumophila (1.9). This pattern of pneumonia is, however, seen with other pathogens and other patterns can be seen in patients with pneumonia due to Legionella pneumophila (see Table 1.1).
A 79-year-old presented with cavitating right upper lobe pneumonia due to Klebsiella pneumoniae. Note that on the chest radiographs (1.10A, B) there is lobar enlargement with the bulging fissure sign (the minor fissure is inferiorly displaced due to the increased volume of the right upper lobe). This pattern of pneumonia is commonly seen with Klebsiella pneumoniae, but can be seen with other virulent organisms such as Staphylococcus aureus and Pseudomonas species.
A 21-year-old male presented with diffuse interstitial shadowing due to Mycoplasma pneumoniae (there were no risk factors for immunodeficiency). There is diffuse reticulonodular shadowing throughout the lung fields, which is particularly noticeable on the chest radiograph (1.11) in the intercostal spaces. Interstitial pneumonia in the immunocompetent host can be seen in viral pneumonias, such as adenovirus, influenza or varicella, and in pneumonias due to ‘atypical pathogens’, such as Mycoplasma and Chlamydia pneumoniae. Note that other patterns of pneumonia can occur with these pathogens (see Table 1.1).
1.9 Chest radiograph showing bilateral pneumonia (arrows) due to Legionella pneumophila.
A 35-year-old male presented with varicella pneumonia. There are diffuse ill-defined foci of air space disease (predominantly nodular shadowing is seen in this film) (1.12). This was associated with disseminated skin lesions of chickenpox.
1.10A, B Chest radiographs (A: PA; B: lateral) showing cavitating right upper lobar pneumonia due to Klebsiella pneumoniae. Note that on the chest radiographs there is lobar enlargement with the bulging fissure sign (arrows). (Courtesy of Dr. D. Patel, Consultant Radiologist, Royal Infirmary, Edinburgh, Scotland.)
1.11 Chest radiograph showing interstitial pneumonia due to Mycoplasma pneumoniae.
1.12 Chest radiograph showing nodular shadowing due to varicella pneumonia (one area is arrowed). (Courtesy of Dr. A. Wightman, Consultant Radiologist, Royal Infirmary, Edinburgh, Scotland.)
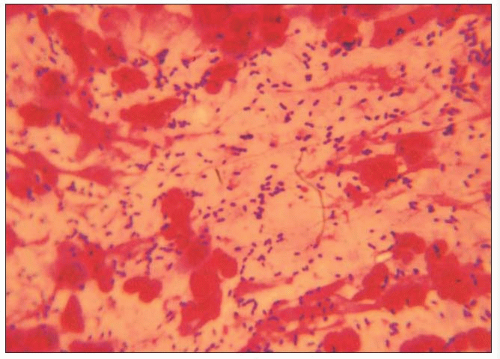
1.13 Gram stain of expectorated sputum sample from a patient with pneumococcal lobar pneumonia, showing Gram-positive diplococci.
Tests available to determine microbiological aetiology
Attempts should be made to establish a specific microbial aetiology in all cases of severe pneumonia. The following tests are useful:
Expectorated sputum (when available) and blood cultures should be obtained before antibiotic therapy is started.
Induced sputum or bronchoalveolar lavage should be considered when expectorated sputum is not available or when Legionnaire’s disease is suspected.
Pleural fluid, if aspirated, should be sent for microscopy and culture, including culture for Legionella.
In patients who have already received antibiotics, tests for pneumococcal capsular antigen may be performed on sputum, blood, or urine samples.
Urine can be sent for Legionella antigen testing.
Acute serum sample can be taken for testing for respiratory viruses and atypical pathogens.
Figures 1.13,1.14,1.15,1.16,1.17,1.18,1.19,1.20,1.20,1.21,1.22,1.23,1.24,1.25 show cultures and staining of organisms in pneumonia. A Gram stain of expectorated sputum sample from a patient with pneumococcal lobar pneumonia is shown (1.13); Gram-positive cocci in pairs are present (diplococci), presumed to be Streptococcus pneumoniae. The sputum sample in 1.13 was cultured on blood agar (1.14). This shows colonies of Streptococcus pneumoniae after 18 hours’ incubation at 37°C.
Only gold members can continue reading. Log In or Register to continue