Coffee is the most widely consumed beverage worldwide and is only second to water drinking and is consumed by 83% of adults in the United States. The long-held controversy regarding the association of coffee consumption with an increased incidence of cardiovascular diseases (CVDs) and hypertension has been reversed by several recent prospective cohort studies and meta-analyses, which have demonstrated that coffee consumption is not associated with increased incidence of CVDs and hypertension and instead it could have a beneficial effect. To get a better understanding of the effects of coffee consumption on cardiovascular health, a Medline search of the English language literature was conducted from 2010 to early 2015 and 25 pertinent reports with information on the effects of coffee drinking, the incidence of CVDs, and hypertension and its mechanism of action were selected for inclusion in this commentary. These studies have shown either a neutral or beneficial effect of coffee on cardiovascular health. In conclusion, coffee is safe to drink by both normal subjects and by those with preexisting CVDs and hypertension.
Coffee is the most widely consumed beverage, second only to water, and in the United States, it is consumed by 83% of adults. There has been a long-standing controversy regarding the association of coffee consumption with the incidence of cardiovascular diseases (CVDs) and hypertension. This controversy was primarily because of older, not well-controlled studies, which demonstrated a positive association of coffee drinking with the incidence of CVDs, hypertension, and type 2 diabetes mellitus. However, according to a major meta-analysis of the older studies, the evidence for the adverse health effects of coffee consumption was based on case-control studies and not on long-term prospective studies, which showed either a neutral or beneficial effect of coffee consumption with CVDs and hypertension. This aspect has been strengthened by recent well-controlled studies, which have demonstrated a beneficial effect of chronic coffee drinking on CVDs and hypertension. To get a better understanding of the beneficial health effects of coffee consumption, a Medline search of the English language literature was conducted from 2010 to early 2015, and of the 93 abstracts reviewed, 25 pertinent reports with data on coffee consumption, its effect on CVDs and hypertension, and the mechanism for this beneficial effect were selected. These articles together with collateral reports will be discussed in this commentary.
Studies Demonstrating a Neutral or Beneficial Effect of Coffee Consumption on CVDs and Blood Pressure
Several recent studies and reviews of prospective and randomized studies involving a large number of subjects have demonstrated a beneficial or neutral effect of coffee consumption on CVD, hypertension, heart failure (HF), stroke, and all-cause mortality. The findings from the most recent studies are summarized in Table 1 . Regarding BP control, 5 studies, 3 large reviews involving 1,502.218, 172,567, and 170,734 subjects and 2 smaller studies, 1 cross-sectional of 836 subjects and 1 prospective cohort study of 2,442, showed either a beneficial or neutral effect of coffee consumption. Of these studies, 1 review and meta-analysis showed that caffeine administration acutely and temporarily increases BP in caffeine-naive hypertensive subjects, whereas another prospective cohort study showed an adverse interaction of high coffee intake with weight and age with SBP for male but not female subjects. With respect to the incidence of CVD, CHD, stroke, HF, and all-cause mortality, several prospective control studies and 2 large reviews and meta-analyses of 170,320 and 1,279,804 patients showed either a neutral of beneficial dose-dependent effect of coffee consumption. Of major significance is a recent prospective cohort study of 402,260 subjects, which showed a beneficial effect of chronic coffee consumption on all-cause and cause-specific mortality after 13 years of follow-up. Similarly, 4 other studies, 3 prospective cohort studies and 1 meta-analysis of 479,689 subjects, showed either a beneficial or neutral effect of coffee consumption. With respect to the incidence of HF, 1 review of 140,220 subjects and 1 prospective cohort study of 59,490 subjects showed either a decrease or a neutral effect of coffee intake.
| Author | Study design | Subjects number | Age years | F-U years | Event type | Change |
|---|---|---|---|---|---|---|
| Guessous | C-S | 836 | 47.8 | na | SBP | ↓ |
| Steffen | Rev | 1,502,218 | 26-55 | 6-33 | BP | ↔ |
| Zhang | Rev | 172,567 | 26-55 | 6-33 | BP | ↓ |
| Griggey | P-C | 2,442 M | 52.1 | 0-41 | SBP | ↔ |
| Mesas | Rev,Meta | 364 | na | 2-8 wks | BP | ↔ |
| Rev,Meta | 170,320 | 30-83 | 4-25 | CVD | ↔ | |
| Liu ∗ | P-C | 43,727 | 43.4 | 17 | all-cause death ∗ | ↑ |
| Freedman | P-C | 402,260 | 50-71 | 13 | all-cause death | ↓ |
| deKoning Gans | P-C | 37,514 | 46-52 | 13 | CHD,Death | ↓ |
| Ding | Rev,Meta | 1,279,804 | 20-83 | 2-32 | CVD,Death | ↓ |
| Sugiyama | P-C | 37,742 W | 40-64 | 10 | CVD,Death | ↓ |
| Lopez-Garcia | P-C | 11,697 W | 62-68 | 24 | CVD,Death | ↔ |
| Floegel | P-C | 42,659 | 49-63 | 9 | CHD,Stroke | ↔ |
| Kokubo | P-C | 82,369 | 45-74 | 3 | CVD,Stroke | ↓ |
| Larsson | Rev,Meta | 479,689 | 20-75 | 2-3 | Stroke | ↓ |
| Mostofsky | Rev | 140,220 | 25-83 | na | HF | ↓ |
| Wang | P-C | 59,490 | 25-74 | 19.2 | HF | ↔ |
∗ Indicates that CVD and all-cause mortality occurred only in high coffee drinkers.
Pathophysiological Mechanism for the Beneficial Effects of Coffee Consumption
Caffeinated coffee
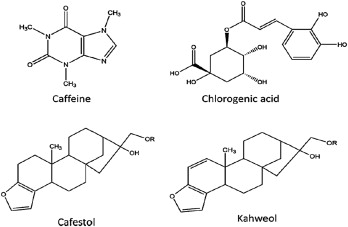
Caffeinated coffee is a complex beverage containing >1,000 compounds among which the most important are caffeine, diterpene alcohols, and chlorogenic acids. On ingestion, caffeine is rapidly absorbed through the gastrointestinal tract and achieves a T max within 30 to 45 minutes. Subsequently, it is metabolized in the liver by the enzyme CYP1A2 into 3 metabolites, paraxanthine, theobromine, and theophylline, with paraxanthine being the most active metabolite. Caffeine exerts its hemodynamic effects through a complex interference with the action of adenosine on its receptors A1 and A2a. Adenosine is an adenine nucleoside that is produced from the hydrolysis of adenosine triphosphate and exerts its hemodynamic effects on the heart and other vascular beds through stimulation of its receptors A1 and A2a. The effects exerted by the receptors A1 and A2a are opposite. Stimulation of A1 receptor causes vasoconstriction of the afferent renal arterioles leading to decrease in glomerular filtration rate and renal blood flow and an increase in renal sodium reabsorption. In contrast, stimulation of A2a receptors causes vasodilation in most vascular beds including the efferent renal arteriole, but the action on the A1 receptors over-rides the adenosine action on the A2a receptors, and the net effect is vasoconstriction. Blockade by caffeine of the A1 receptors localized in the afferent arteriole, glomerulus, proximal tubule, and collecting ducts improves glomerular filtration rate and renal blood flow and causes diuresis and natriuresis and lowers the BP. These actions of adenosine inhibitors have been shown to improve the condition of patients with HF by improving renal function and enhancing the action of diuretics. Besides receptors A1 and A2a, 2 more adenosine receptors, A2b and A3, with vasodilatory properties have been identified, but their significance is not clearly known. Other mechanisms by which coffee could lower the BP are through the caffeine metabolites ( Figure 1 ), among which are the chlorogenic acids contained in the coffee. Chlorogenic acids are potent antioxidants and improve endothelial and vascular function through increased availability of nitric oxide.