Due to their remarkable reduction of the need for subsequent revascularization, and yet despite the fact that drug-eluting stents (DES) have not been shown to improve long-term patient survival or freedom from myocardial infarction (MI), the use of DES has been very warmly embraced by the interventional community. Most U.S. centers report utilization in approximately 90% of their stentreceiving patients. For the physician in the relatively costunconstrained environment, the principal question then becomes “For whom are DES contraindicated on the basis of increased risk?” For the physician operating in an environment where there is more focus on cost, an additional important question is “For whom are DES relatively contraindicated due to marginal ‘value’?”
The field of DES continues to evolve. Despite several moderate-sized randomized trials and registries, important questions germane to the question of who should receive DES remain. Several reports now highlight the small but significantly increased hazard of late stent thrombosis with the utilization of DES compared to bare metal stents (BMS). The absolute increase appears to be about 0.5% between 6 and 24 months after stenting (1). This seems to occur principally during periods of antiplatelet therapy withdrawal, and especially during the stress of surgery. The exact risk for such patients is difficult to ascertain at present, due to our inexact knowledge of precisely which medications patients are taking long after enrollment into randomized trials, but the risk may be as high as 5% with dual antiplatelet therapy withdrawal for periods of a week or more in conjunction with the stress of noncardiac surgery (2). Whether or not both CYPHER and TAXUS stents pose equal risk has not been clarified yet. Early reports suggest also that patients resistant to aspirin, clopidogrel, or both also are at increased risk (3). If validated, and particularly if these tests can be standardized, these reports suggest that patients considered for elective DES use should have resistance to antiplatelet medications tested before stent implantation. These populations represent, then, the principal group for whom DES may well be contraindicated. To this group, of course, must be added those occasional patients who are truly allergic to either sirolimus or paclitaxel.
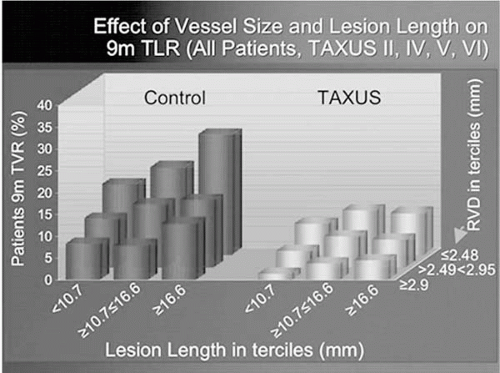
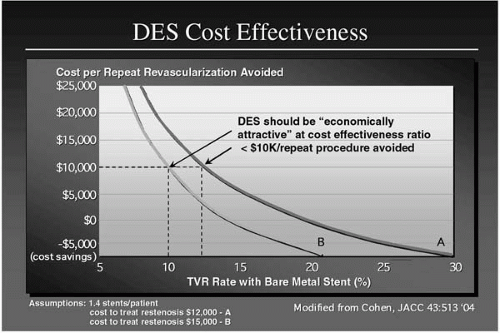
The cost-effectiveness of DES relates principally to the absolute magnitude of reduction in clinical restenosis. Generally speaking, DES reduce restenosis to a relatively equal extent across various patient populations; hence absolute reduction in risk is directly related to initial risk with BMS. This is known to be particularly high in patients with diabetes, long lesions, small reference dimensions, previous restenosis at the treatment site, and saphenous vein graft (SVG) intervention. Conversely, in the absence of these findings, the relative benefit is diminished. This can be seen graphically in the target vessel revascularization (TVR) rate versus lesion length/reference vessel diameter graft from the Taxus series (4) (Fig. 15A.1) and more formally in the work from Cohen (5) depicted in Figure 15A.2.
Another group of patients for whom DES may be relatively contraindicated are those patients who, by virtue of complex intervention and the location of the lesion, may be at greater risk of subacute thrombosis (SAT), with catastrophic results. This would include, in particular, patients undergoing “crush” or other high metal/polymer/drug density bifurcation intervention in the distal left main (when that vessel is unprotected) and in the proximal left anterior descending (LAD)/large diagonal setting. The approximate doubling of SAT risk in this setting must be balanced against the benefit of reducing restenosis.
Figure 15A.1.
In summary, the physician operator should generally elect to utilize DES in preference to BMS except when the risk of stent thrombosis is particularly high or when the relative clinical benefit with regard to clinical restenosis reduction is marginal. We have considerably more data regarding the latter issue than the former. Whether we can better identify patients at heightened SAT risk utilizing aspirin or clopidogrel resistance, or perhaps specific forms of genetic testing, remains to be ascertained.
Figure 15A.2.
REFERENCES
1. Stone GW. Meta-analysis of TAXUS II, IV, V and VI studies. Presented at Boston Scientific evening symposium at the Annual Scientific Session (ACC) 2005, March 7, Orlando, Florida.
2. Ong TL, McFadden EP, Regar E, et al. Late angiographic stent thrombosis (LAST) events with drug-eluting stents. J Am Coll Cardiol 2005 (submitted).
3. Hoffmann S, Klamroth R, Landgraf H, et al. Clopidogrel resistance, ASA resistance and coronary stent thrombosis: a causal relation? J Am Coll Cardiol 2005;45:87A;868.
4. Stone G. Outcomes of the polymer-based, paclitaxel-eluting TAXUS stent in complex lesions. Presented at Annual Scientific Session (ACC) 2005, March 6-9, Orlando, Florida.
5. Greenberg D, Bakhai A, Cohen DJ. Can we afford to eliminate restenosis? Can we afford not to? J Am Coll Cardiol 2004;43:513.
B GENERAL PATIENT SELECTION
Ryan D. Christofferson
Mark Reisman
Restenosis is not a benign condition. Although it does not carry an increased mortality risk (1), recurrent angina and repeat revascularization resulting from restenosis decrease quality of life and erode patient satisfaction, while adding significantly to health care expenditure (2). It has persisted as the Achilles’ heel of percutaneous coronary intervention (PCI), affecting about one-third of all PCI patients (3), and limiting the application of PCI in lesion subsets with unacceptably high rates of restenosis. Despite a long history of failed innovations to prevent restenosis, the recent development of drug-eluting stents (DES) has revolutionized the application of PCI by achieving previously unseen reductions in the rate of restenosis (4,5). The resulting paradigm shift has been compared to the transition from balloon angioplasty (BA) to coronary stenting in terms of its magnitude (6). However, the universal application of DES is currently limited by high DES cost (7) and lack of published evidence in so-called “real world” patient cohorts and complex lesion subsets (8). Because of these limitations, the selective use of DES is currently advocated by some authors (9).
The purpose of this review is to discuss patient and lesion subsets likely to benefit or be harmed by DES, and to provide a framework for rational patient selection for DES use. A number of different stent platforms have been compared to bare metal stenting (BMS) in randomized, controlled trials; however, only sirolimus- (Cypher, Cordis) and paclitaxel- (Taxus, Boston Scientific) eluting stents have achieved U.S. Food and Drug Administration (FDA) approval and widespread use. This review focuses only on peer-reviewed publications regarding paclitaxeland sirolimus-eluting stents.
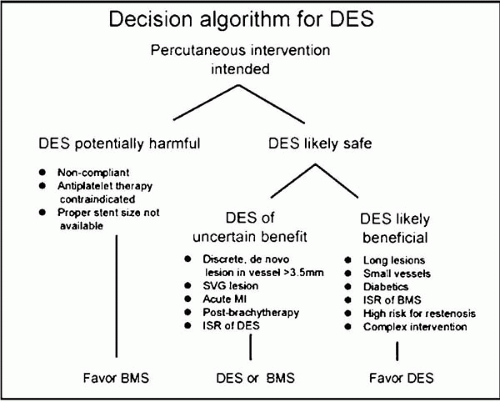
Figure 15B.1. Suggested decision algorithm for DES use.
RATIONAL STRATEGY FOR PATIENT SELECTION FOR DRUG-ELUTING STENTS
Patients experiencing an unacceptably high rate of in-stent restenosis (ISR) represent the target population for DES. In particular, patients with diabetes, prior restenosis, chronic occlusions, and long or complex lesions in small vessels have an increased risk of restenosis with BMS (3,10,11). Additionally, patients who undergo complex or high-risk intervention (e.g., bifurcation lesions, unprotected left main, proximal left anterior descending [LAD] lesions) may be at an increased risk of adverse consequences from restenosis. DES selection in an individual patient should incorporate that patient’s risk factors for restenosis, the significance of restenosis should it occur, and the evidence that DES can be applied safely. Noncompliance, contraindication to antiplatelet therapy, or improper stent size should prohibit DES use. Cost-effectiveness of DES currently must also be considered. A suggested decision algorithm for DES use is shown in Figure 15B.1.
TABLE 15B.1. RANDOMIZED TRIALS OF SIROLIMUS AND PACLITAXEL-ELUTING STENTS
Several randomized, controlled trials (listed in Table 15B.1) have been reported on the use of DES (4,5,12, 13, 14, 15, 16, 17). All these trials (except TAXUS I, which allowed restenotic lesions) enrolled patients with single, de novo lesions in native coronary vessels. Early feasibility trials (4,5,12) mandated that a single stent be used, and target lesions were generally discrete in length (<12 to 18 mm). Later landmark trials (13,15) included longer lesions (15 to 32 mm) and allowed one to two stents. Typical angiographic exclusion criteria in these studies included left main or ostial lesions, moderate to severe calcification, bifurcation lesions, thrombus-containing lesions, and total occlusions. Clinical exclusion criteria typically included acute myocardial infarction (MI), prior brachytherapy, low ejection fraction (<25%), and contraindication to antiplatelet therapy. DESs were clearly superior to BMSs in these trials, with remarkable reductions of approximately 80% in revascularization rates.
A true paradigm shift with regard to restenosis risk has occurred subsequent to the randomized trials and subgroup analyses of DES use. Traditional risk factors for restenosis appear to play a significantly reduced role or no role in the development of restenosis with DES. In fact, the TAXUS IV investigators concluded that diabetes, lesion length, and reference vessel diameter did not play a role in the development of restenosis with paclitaxel-eluting stents (15). Multivariate analysis from the SIRIUS trial, as well as subsequent registry data, have found that with sirolimuseluting stents, the above-mentioned traditional risk factors for ISR still predict restenosis (13,18,19). The relative benefit of sirolimus-eluting stents, however, has been shown to be greater in these patients because of the relatively higher rate of restenosis with BMS (18). Restenosis with DES appears to depend more on technical or mechanical factors, including geographical miss from low or high stent-toartery ratio, incomplete coverage of the lesion, edge effect, and the presence of gaps between stents.
Limitations of the Randomized Trials
The criticism of the randomized trial data is that patients in the trials had simple, relatively discrete, de novo lesions in native coronary arteries, which is only a subset of the patients in real-world conditions. Very few patients with complex lesions (AHA/ACC type C) were included in the published randomized trials. Results soon will be available from the latest paclitaxel trial, TAXUS VI, which includes a much higher percentage of type C lesions. Preliminary results for this trial have indicated that, even in complex lesion subsets, a substantial reduction in restenosis occurs with paclitaxel-eluting stents. Concern also exists that the randomized trials did not have adequate follow-up duration to detect a “catch-up” phenomenon with DES, in which restenosis is merely delayed by DES and not eliminated, similar to findings with vascular brachytherapy. Early feasibility studies, however, have reported long-term follow-up at 2 years and have failed to detect any evidence of late restenosis (20,21).
TABLE 15B.2. RECOMMENDED GUIDELINES FOR DES USE IN SPECIFIC LESIONS AND SUBSETS
I
1. De novo lesions <32 mm, RVD 2.25 to 3.75 mm with 50% to 99% preprocedure (A) (4,5,12, 13, 14, 15, 16,22)
2. Contraindication to antiplatelet therapy (C) (43)
Limited to sirolimus- and/or paclitaxel-eluting stents.
Classification of Recommendations
Level of Evidence
I
Intervention is useful and effective
IIa
Weight of evidence/opinion is in favor of usefulness/efficacy
A
Data from many large, RCTs
B
Data from fewer, smaller RCTs, careful analyses of nonrandomized studies, observational registries
IIb
Usefulness/efficacy is less well established by evidence/opinion
III
Intervention is not useful/effective and may be harmful
C
Expert consensus
LESION-SPECIFIC DES STENTING
Several registry and case-control studies have been intended to assess for DES safety and efficacy in specific lesion subsets not included in the randomized trials. Table 15B.2 lists some suggested guidelines, adapted from O’Neill et al. (8), which may be useful to guide clinicians considering off-label DES use in more complex patient subsets.
Of special interest is the management of ISR. A retrospective analysis of the First-in-Man (FIM) registry found no difference in late loss or percent diameter stenosis at 6 months between patients with ISR and de novo lesions (24). Sousa et al. found similar results in a review of 25 patients with ISR receiving a sirolimus-eluting stent, with only one patient in the study developing angiographic ISR at 1-year follow-up (23). Traditionally, vascular brachytherapy has been the treatment of choice for complex ISR. Radke et al., in a case-control study, compared paclitaxel-eluting stents to brachytherapy and found no difference in binary restenosis and target lesion revascularization at 12 months (25). Similar results were found when sirolimuseluting stents were compared to vascular brachytherapy (26). Further randomized trial data is needed to definitively answer this question.
Only gold members can continue reading. Log In or Register to continue