Fig. 3.1
Complete heart block
Cardiac sarcoidosis may be mis-diagnosed as arrhythmogenic right ventricular cardiomyopathy (ARVC) [1, 5–7]. Cardiac sarcoidosis should be considered in patients with non-ischemic cardiomyopathy, left ventricular systolic dysfunction and congestive heart failure. Congestive heart failure is the second most common cause of death, following sudden cardiac death, in patients with cardiac sarcoidosis.
Valvular dysfunction most often involves the mitral valve, and is more commonly due to papillary muscle dysfunction as a result of myocardial involvement (Fig. 3.2). Pericardial effusion may occur, and the first reported case of cardiac sarcoidosis was that of pericardial granulomas [8].
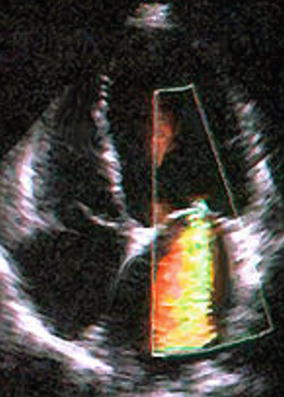
Fig. 3.2
Severe mitral regurgitation in a 56 year old sarcoidosis patient
Patients with cardiac sarcoidosis may present with a variety of non-specific symptoms including palpitations, chest pain, and dyspnea. The electrocardiogram may be abnormal in up to 50 % of patients with sarcoidosis without clinically evident cardiac involvement [1, 4]. These abnormalities may be mild and non-specific such as a fragmented QRS complex, atrio-ventricular block or bundle branch block [9, 10]. A patient with sarcoidosis and possible cardiac related symptoms or any abnormality on the electrocardiogram should under go further evaluation for cardiac sarcoidosis.
Because there is no “gold standard” test for cardiac sarcoidosis and serious or life threatening complications may be the initial clinical presentation, keeping a high index of suspicion and a low threshold to pursue evaluation for possible cardiac involvement in patients with sarcoidosis is imperative.
Pearls of Wisdom
1.
There is no gold standard test for cardiac sarcoidosis.
2.
< div class='tao-gold-member'>
Clinical presentations vary from no clinically noticeable symptoms to marked dyspnea, syncope, fatigue and more.
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


