Chapter 16
Chronic Stable Angina
1. Can a patient with new-onset chest pain have chronic stable angina?
2. What causes chronic stable angina?
3. How is chronic stable angina classified or graded?
The most commonly used system is the Canadian Cardiovascular Society system, in which angina is graded on a scale of I to IV. These grades and this system are described in Table 16-1. This grading system is useful for evaluating functional limitation, treatment efficacy, and stability of symptoms over time.
TABLE 16-1
GRADING OF ANGINA BY THE CANADIAN CARDIOVASCULAR SOCIETY CLASSIFICATION SYSTEM
Class I


Class II

 Angina occurs while walking or climbing stairs rapidly; while walking uphill; while walking or climbing stairs after meals in cold or in wind; while under emotional stress; or only during the first several hours after waking.
Angina occurs while walking or climbing stairs rapidly; while walking uphill; while walking or climbing stairs after meals in cold or in wind; while under emotional stress; or only during the first several hours after waking.
 Angina occurs while walking > 2 blocks on level grade and climbing > 1 flight of ordinary stairs at a normal pace and in normal conditions.
Angina occurs while walking > 2 blocks on level grade and climbing > 1 flight of ordinary stairs at a normal pace and in normal conditions.
Class III

 Angina occurs while walking 1 or 2 blocks on level grade and climbing 1 flight of stairs in normal conditions and at a normal pace
Angina occurs while walking 1 or 2 blocks on level grade and climbing 1 flight of stairs in normal conditions and at a normal pace
Class IV


4. What tests should be obtained in the patient with newly diagnosed angina?
5. What are the goals of treatment in the patient with chronic stable angina?

 Prevent major cardiovascular (CV) events, such as heart attack or cardiac death
Prevent major cardiovascular (CV) events, such as heart attack or cardiac death
 Identify “high risk” patients who would benefit from revascularization
Identify “high risk” patients who would benefit from revascularization
6. What therapies improve symptoms?




7. What is the initial approach to the patient with chronic stable angina?
The initial approach should be focused on eliminating unhealthy behaviors such as smoking and effectively promoting lifestyle changes that reduce CV risk, such as maintaining a healthy weight, engaging in physical activity, and adopting a healthy diet. In addition, annual influenza vaccination reduces mortality (by approximately 35%) and morbidity in patients with underlying CAD. Tight glycemic control was thought to be important in the diabetic, but this approach actually increases the risk of CV death and complications.
8. What is first-line drug therapy for the treatment of stable angina?
9. Is any β-blocker better than the others?
Although the various β-blockers have different properties (i.e., cardioselectivity, vasodilating actions, concomitant α-adrenergic inhibition, and partial β-agonist activity [Table 16-2]), they appear to have similar efficacy in patients with chronic stable angina. β-blockers prevent reinfarction and improve survival in survivors of MI, but such benefits have not been demonstrated in patients with chronic CAD without previous MI.
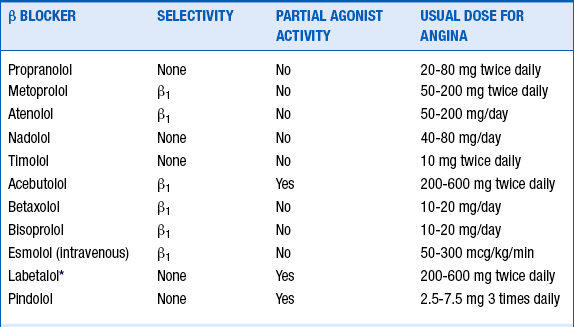
10. What is the proper dose of β-blocker?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


