Chest Wall Invasive Diseases
Toms Franquet, MD, PhD
DIFFERENTIAL DIAGNOSIS
Common
Primary Tumors
Lung Cancer
Mesothelioma
Metastases
Less Common
Actinomycosis
Empyema Necessitatis
Tuberculosis
Primary Rib Tumors
Chondrosarcoma
Osteosarcoma
Lymphoma
Soft Tissue Sarcomas
Fibrosarcoma and Malignant Fibrohistiocytoma
Rare but Important
Primary Chest Wall Infection: Necrotizing Fasciitis
Primitive Neuroectodermal Tumor (Askin Tumor)
Deep Fibromatoses
Aggressive Fibromatosis
Musculoaponeurotic Fibromatoses
Desmoid Tumors
Sternal Osteomyelitis
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Consider clinical presentation, natural history, and patient age at presentation
Empyema necessitatis: Fluid collections in pleura and chest wall
Necrotizing fasciitis
Signs of inflammation may not be apparent (early stage) if bacteria are deep within soft tissues
Subcutaneous air (gas-forming organisms) commonly present
Chondrosarcoma is most common malignant primary bone tumor of chest wall in adults
Soft tissue sarcomas are indeterminate by imaging features
Fibromatosis may be component of Gardner syndrome (familial adenomatous polyposis)
Helpful Clues for Common Diagnoses
Lung Cancer
Pancoast tumor: Traverses lung apex and may involve lower trunks of brachial plexus
May involve pleura, intercostal nerves, adjacent ribs, and vertebrae
Findings of invasion: Rib destruction, encasement of nerves or blood vessels
Mesothelioma
Circumferential pleural involvement (including mediastinal pleura)
Pleural fluid 95%
CT findings of chest wall invasion: Obscuration of fat planes, infiltration of intercostal muscles, periosteal reaction, and bone destruction
May also invade mediastinum and diaphragm
Metastases
Frequent history of primary tumor
Common primaries: Lung, kidney, breast, and prostate
Helpful Clues for Less Common Diagnoses
Actinomycosis
Rod-shaped bacterium, anaerobe, sulfur granules
Traverses fascial planes from lung to pleura to chest wall
May create fistulas
Empyema Necessitatis
Mycobacterium tuberculosis
Contiguous spread from underlying pleural or pulmonary lesions
May create fistulas
Primary Rib Tumors
Chondrosarcoma, osteosarcoma
Lesions can be osteolytic, osteoblastic, or both
Scattered flocculent calcifications
Large lobulated excrescent mass arising from rib
Chest wall extension: Soft tissue mass
Lymphoma
Direct extension into anterior chest wall from anterior mediastinal lymph nodes
Isolated chest wall lesions without direct extension can occur
Chest wall mass with rib destruction: Lytic or sclerotic
May grow around sternum or ribs without destroying them
Soft Tissue Sarcomas
Fibrosarcoma and malignant fibrohistiocytoma
Malignant fibrous histiocytoma: Most common malignant soft tissue sarcoma in adults
Similar CT and MR appearances
Helpful Clues for Rare Diagnoses
Primary Chest Wall Infection: Necrotizing Fasciitis
Rapidly spreading infection of subcutaneous tissue
Uncommon but potentially fatal condition
Tissue necrosis and gas formation
Spontaneous or in patients with diabetes, immunosuppression, post trauma, or surgery
Staphylococcus aureus, Pseudomonas aeruginosa
Primitive Neuroectodermal Tumor (Askin Tumor)
Large chest wall mass in adolescent or young adult
Rib destruction, pleural thickening or pleural effusion and focal invasion of lung
MR should be performed to delineate soft tissue involvement
Deep Fibromatoses
Aggressive fibromatoses
Can be very large with high tendency to recur after treatment
Rarely intrathoracic
CT features: Enhancing soft tissue mass that may be iso- or slightly hypodense to surrounding muscle
MR features: Isointense on T1-weighted images and heterogeneously hyperintense on T2-weighted images; shows bands of low signal on all sequences
Musculoaponeurotic fibromatoses
Chest wall involvement (10-28%)
Solitary or multicentric
Desmoid tumors
Soft tissue masses with poorly defined margins
Most frequently located in abdomen (50%)
Chest wall (8-10%)
Very rarely intrathoracic
Sternal Osteomyelitis
Primary
Intravenous illicit drug users
Secondary
After median sternotomy for cardiac surgery (0.5-5%)
CT is imaging method of choice
CT features: Irregularity of bony sternotomy margins, bony sclerosis, and peristernal soft tissue masses with abscess formation
Image Gallery
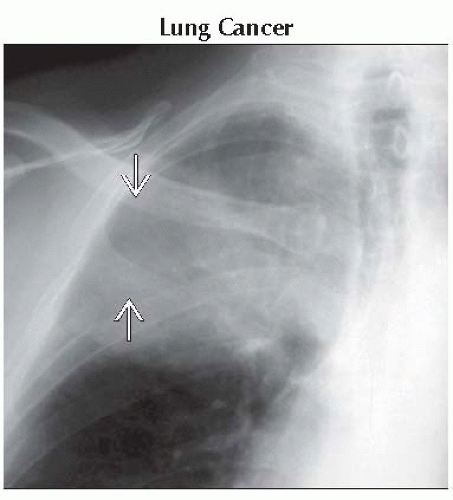 Anteroposterior radiograph shows a large opacity in the upper part of the right hemithorax. Osteolysis of the 3rd and 4th ribs  is also seen in this patient with Pancoast tumor. is also seen in this patient with Pancoast tumor. |
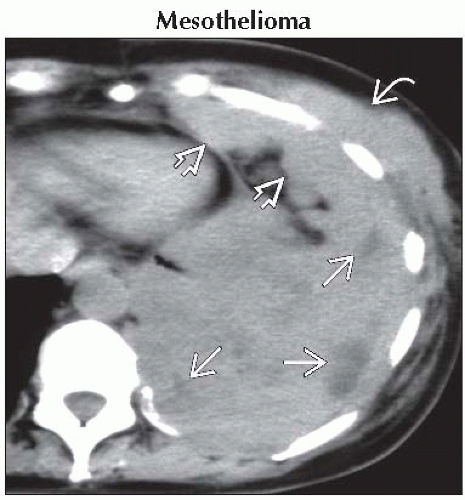 Axial NECT shows a large heterogeneous mass with areas of necrosis
 in the left hemithorax. Diffuse nodular pleural thickening in the left hemithorax. Diffuse nodular pleural thickening  and chest wall infiltration and chest wall infiltration  is seen. is seen.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|