Chapter 4
Chest Radiographs
1. Describe a systematic approach to interpreting a chest radiograph (chest x-ray [CXR]) (Fig. 4-1).
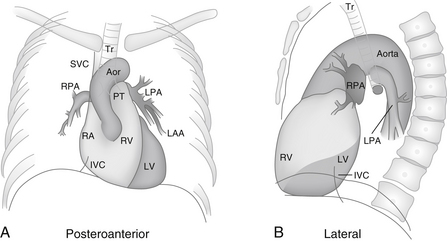
Figure 4-1 Diagrammatic representations of the anatomy of the chest radiograph. A, Aor, Aorta; IVC, inferior vena cava; LAA, left atrial appendage; LPA, left pulmonary artery; LV, left ventricle; PT, pulmonary trunk; RA, right atrium; RPA, right pulmonary artery; RV, right ventricle; SVC, superior vena cava; Tr, trachea. B, IVC, inferior vena cava; LPA, left pulmonary artery; LV, left ventricle; RPA, right pulmonary artery; RV, right ventricle; Tr, trachea. (From Inaba AS: Cardiac disorders. In Marx J, Hockberger R, Walls R, editors: Rosen’s emergency medicine: concepts and clinical practice, ed 6, Philadelphia, 2006, Mosby.)
Common recommendations are to:
1. Begin with general characteristics such as the age, gender, size, and position of the patient.
2. Next, examine the periphery of the film, including the bones, soft tissue, and pleura. Look for rib fractures, rib notching, bony metastases, shoulder dislocation, soft tissue masses, and pleural thickening.
3. Then, evaluate the lung, looking for infiltrates, pulmonary nodules, and pleural effusions.
4. Finally, concentrate on the heart size and contour, mediastinal structures, hilum, and great vessels. Also note the presence of pacemakers and sternal wires.
2. Identify the major cardiovascular structures that form the silhouette of the mediastinum (Fig. 4-2)
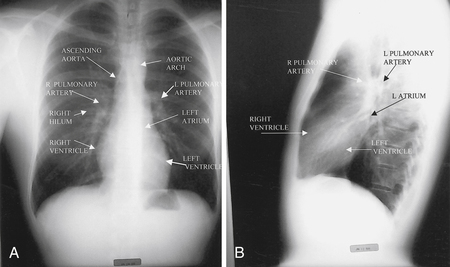
 Right side: Ascending aorta, right pulmonary artery, right atrium, right ventricle
Right side: Ascending aorta, right pulmonary artery, right atrium, right ventricle
 Left side: Aortic knob, left pulmonary artery, left atrial appendage, left ventricle
Left side: Aortic knob, left pulmonary artery, left atrial appendage, left ventricle
3. How is heart size measured on a chest radiograph?
4. What factors can affect heart size on the chest radiograph?
 Size of the patient: Obesity decreases lung volumes and enlarges the appearance of the heart.
Size of the patient: Obesity decreases lung volumes and enlarges the appearance of the heart.
 Degree of inspiration: Poor inspiration can make the heart appear larger.
Degree of inspiration: Poor inspiration can make the heart appear larger.
 Emphysema: Hyperinflation changes the configuration of the heart, making it appear smaller.
Emphysema: Hyperinflation changes the configuration of the heart, making it appear smaller.

 Chest configuration: Pectus excavatum can compress the heart and make it appear larger.
Chest configuration: Pectus excavatum can compress the heart and make it appear larger.
 Patient positioning: The heart appears larger if the film is taken in a supine position.
Patient positioning: The heart appears larger if the film is taken in a supine position.

5. What additional items should be reviewed when examining a chest radiograph from the intensive care unit (ICU)?
On portable coronary care unit (CCU) and ICU radiographs, particular attention should be paid to:








A careful inspection should be made for pneumothorax (Fig. 4-3), subcutaneous emphysema, and other factors that may be related to instrumentation and mechanical ventilation.
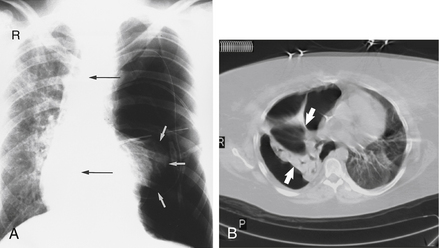
Figure 4-3 Tension pneumothorax. On a posteroanterior chest radiograph (A) the left hemithorax is very dark or lucent because the left lung has collapsed completely (white arrows). The tension pneumothorax can be identified because the mediastinal contents, including the heart, are shifted toward the right (black arrows) and the left hemidiaphragm is flattened and depressed. B,
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


