Fig. 7.1
Selective injection of the CT: thin helicine arteries (typical pattern of cirrhosis), heterogeneous hepatography, and segment VI tumoral hypervascularization
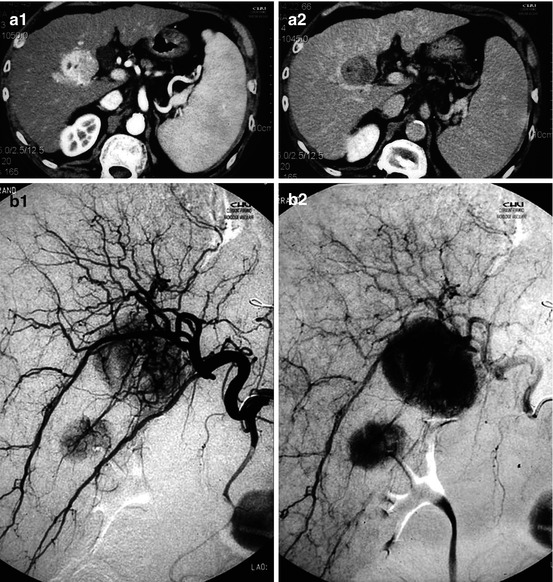
Fig. 7.2
HCC complication of HVC hepatitis. (a) CT, juxta-gallbladder tumor; arterial phase, massive enhancement (wash-in) and then washout on the portal phase scan. (b) Same patient, 2D angio correlation: 2 tumors foci
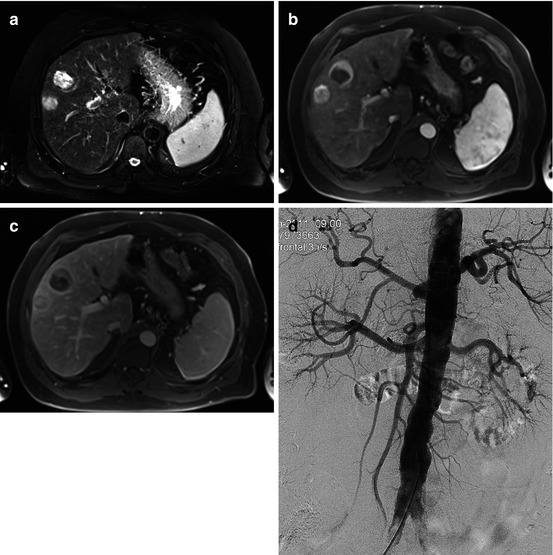
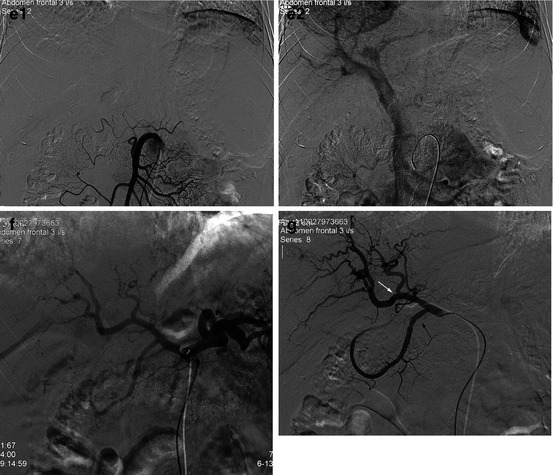
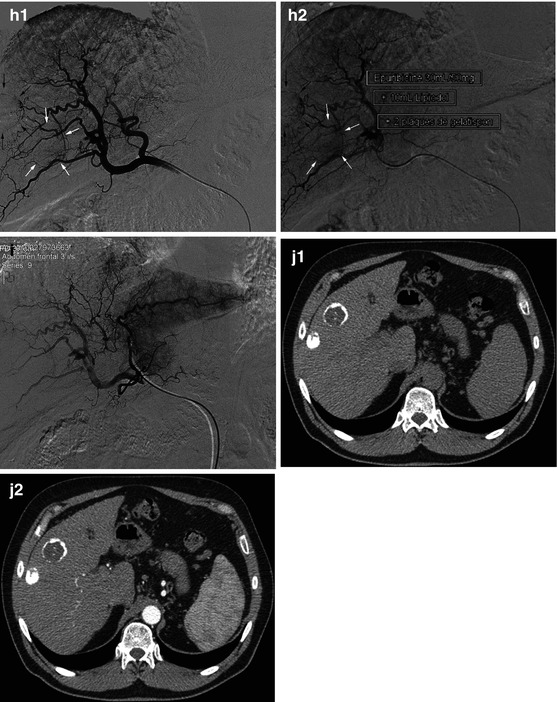
Fig. 7.3
Double HCC; the multidisciplinary concertation and a complete workup led to decide a hepatic transplantation. But a long waiting delay (months) is expected, so an adjuvant TACE has been decided. (a) MRI T2-weighted scan: 25 and 30 mm heterogeneous hypersignal tumors. (b) Dynamic MR, arterial phase: global enhancement of one of this lesion (wash-in) and peripheral enhancement of the other. (c) Late portal phase: washout. (d) Aortography (right femoral access): modal angiographic anatomy of the splanchnic collaterals of the aorta. (e) Selective SMA injections, arterial and venous phase: patent portal vein and hepatoportal flow direction. (f) Selective injection of the CT. (g) Common hepatic A selective injection, just upstream the gastroduodenal A (arrow): unusual distribution of the terminal branches of the proper hepatic A, with an accessory left hepatic artery, and then a right/left bifurcation. (h) Accessory left hepatic artery selective injection, early arterial and late phases: double tumorography. (i) Injection of this accessory hepatic A. TACE: we injected epirubicin 50 mg (25 ml) + Lipiodol (10 ml), 20 % in the accessory branch and 40 % in each of the right and left hepatic branches. 2 × 5 cm3 gelatin sponge syringes were then injected, in order to observe a very slow flow. (j) CT 1 m later: dense Lipiodol fixation in the lesion which was previously massively enhanced and peripheral fixation in the other. No arterial enhancement
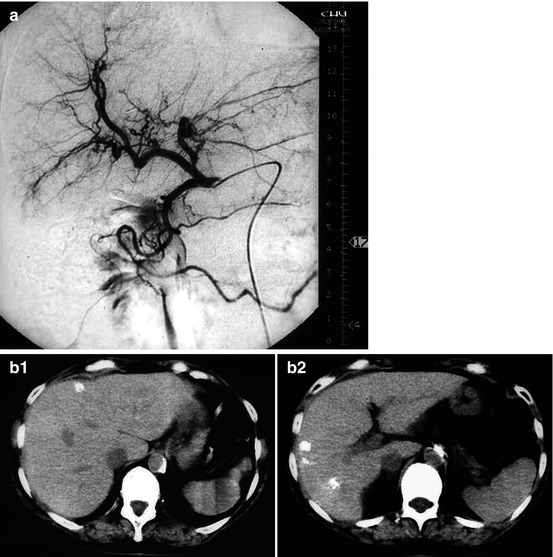
Fig. 7.4
HCC treated by TACE. (a) Selective common hep A injections: nonselective TACE (2/3 in the right hepatic A, 1/3 in the left). (b) 1 m later CT: tumoral Lipiodol fixation
References
1.
2.
Bruix J, Sherman M. Management of hepato cellular carcinoma: an update AASLD practice guidelines. Hepatology. 2010;53:1–34.CrossRef
3.
4.
5.
6.
Mazzafero V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepato cellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334:693–9.CrossRef
7.
Liapi E, Geschwind JF. Intra-arterial therapies for hepatocellular carcinoma: where do we stand? Ann Surg Oncol. 2010;17:1234–46.PubMedCrossRef
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


