Fig. 16.1
Professor Jules Janssen en route to the Grands Mulets (3050 m) on Mont Blanc during a reconnaissance. The difficulties of the route can be seen. From Vivian [24]
Only about three years after the installation of the Observatoire Vallot, Angelo Mosso (1846–1910) who was professor of physiology in Turin arranged for the construction of the Capanna Margherita on one of the peaks of the Monte Rosa. This was extraordinarily high at 4559 m and again access was very difficult involving a long climb over glaciers in a region with hidden crevasses. The hut owes its name to Queen Margherita who was a keen alpinist, and she actually visited the hut soon after its construction and spent the night there. The Capanna Margherita was the site of extensive physiological studies carried out by the burgeoning international high altitude physiology community. Interestingly, Mosso who made many important contributions did not accept Bert’s conclusion that hypoxia was the culprit, but instead Mosso blamed the low carbon dioxide level in the body, a condition that he called acapnia. Another important high altitude physiologist in the early part of the century was Nathan Zuntz (1847–1920) who was a professor of animal physiology in Berlin. In 1910 he organized an important expedition to the Alta Vista Hut (altitude 3350 m), on Tenerife, Canary Islands.
So this was the situation in 1910 when J.S. Haldane (1860–1936) and Yandell Henderson (1873–1944) discussed the possibility of another physiological expedition to high altitude. Haldane (Fig. 16.2) came from a distinguished old Scots family and he attended Edinburgh University where his initial interest was philosophy. Later he turned to medicine but interestingly his first major paper was actually on philosophy [12]. Following graduation he was an instructor at University College, Dundee where he carried out a project on the foul air of the slums of Dundee and reported abnormally high concentrations of carbon dioxide. In 1887 he became a lecturer in physiology in Oxford and in 1905 published with Priestley a landmark paper on the importance of carbon dioxide on the control of ventilation [15]. Haldane’s contributions to physiology were very extensive and went far beyond his interests in high altitude [14]. They included important studies on mine air and decompression sickness and in fact he was a key figure in industrial physiology.
The origin of the Pikes Peak Expedition makes entertaining reading. Haldane met Yandell Henderson, who was a physiologist at Yale University, at the International Congress of Physiology in Vienna in 1910 and the conversation was recounted by Henderson [17]. Haldane remarked that what was needed was “a nice, comfortable mountain”. This sounds rather whimsical but Haldane was referring to the difficult access and the spartan conditions of high altitude stations such as the Observatoire Vallot and the Capanna Margherita. According to Henderson, Haldane stated that to reach the Capanna Margherita “one must climb several thousand feet over snow and ice… the climate is arctic even in midsummer… worst of all the investigator must cook for himself”. He continued, it is “open to question whether the effects observed were due to the barometric pressure… or bad cooking”. In fact Joseph Barcroft (1872–1947), a distinguished high altitude physiologist from Cambridge, had made a similar remark about the Capanna Margherita when he stated “the difficulty of transport greatly restricts the possibilities both of research and gastronomy”.
By contrast Henderson pointed out that Pikes Peak, a mountain outside Colorado Springs in the Rockies, had a number of advantages including easy access via a cog railway, a substantial altitude of 4300 m, several rooms at the hotel on the summit that could be set aside for the expedition, and the possibility of a warm laboratory. Haldane later remarked on the “excellent cuisine”. In other words this venue meant that the effects of high altitude, that is, the sustained hypoxia, could be studied in the absence of complicating factors such as difficult access, limited laboratory instrumentation, severe cold, and poor food that had to be prepared by the investigators. Incidentally the same principles were enunciated by Griffith Pugh (1909–1994) when he planned the Silver Hut Expedition 50 years later in 1960 [21]. In this case a group of physiologists lived at an altitude of 5800 m for several months in a warm environment with ample food.
The design of the Pikes Peak expedition was classical. Physiological measurements were first made at sea level in Oxford or New Haven. Then there was a short period at Colorado Springs altitude 1830 m, where equipment was readied, following which the four investigators Douglas, Haldane, Henderson and Schneider ascended together on the cog railway (Fig. 16.3). They spent five uninterrupted weeks at high altitude studying the changes during acclimatization, and then descended via Colorado Springs back to sea level where further studies were carried out. C.G. Douglas (1882–1963) was a collaborator of Haldane’s in Oxford. E.C. Schneider (1874–1954) had previously been at Yale but at the time of the expedition was on the faculty of Colorado College in Colorado Springs. This was convenient because it meant that supplies or equipment could be brought up from nearby if necessary. An extensive series of projects were carried out on the summit and these will be summarized here. The official report [5] which is easily available from JSTOR is 133 pages long and written in a relaxed leisurely style that modern editors would not condone.
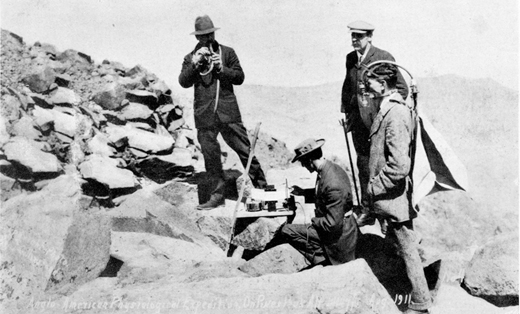
Fig. 16.3
Members of the expedition. From left to right, Henderson taking samples of alveolar gas, Schneider sitting and recording his respiration, Haldane standing, Douglas wearing a “Douglas bag” to collect expired gas for the determination of oxygen consumption during climbing. From Henderson [18]
16.1 Acute Mountain Sickness
All four investigators developed acute mountain sickness shortly after arriving at the summit with headache that was severe at times, loss of appetite, nausea, intestinal disturbances, hyperventilation, cyanosis and periodic breathing. However after 2 or 3 days, most of the symptoms disappeared although the hyperpnea and dyspnea remained as did the periodic breathing in some subjects. Many visitors arrived at the summit by train and some of these showed extreme acute mountain sickness with nausea, vomiting, and fainting. The official description [5] includes “… the scene in the restaurant and on the platform outside can only be likened to that on the deck or in the cabin of a cross-channel steamer during rough weather”.
16.2 Alveolar Gases During Acclimatization
Extensive measurements of the PO2 in alveolar gas and arterial blood were made. Figure 16.4 shows alveolar gas partial pressures from Douglas during the whole period. This is a reproduction of the top panel of Fig. 16.6 in the official report. The results in the other three subjects were similar. Note that after 3 or 4 days in Colorado Springs, the PCO2 fell from the sea level value of about 40 to about 32 mmHg and continued its decline during most of the five weeks ending at a value of about 25 mmHg. Consistent with this the alveolar PO2 fell precipitously to about 50 mmHg on arrival at the summit and then gradually increased over the five week period ending at about 56 mmHg. On descent to Colorado Springs both the PCO2 and PO2 increased, but it is interesting that over the three week period after the expedition when the subjects were in New Haven at sea level, the PCO2 only gradually returned to its normal value of 40. This was a particularly useful finding because there are relatively few data on the deacclimatization process on return to sea level, and in fact these are some of the best data in the literature albeit 100 years old!
Fig. 16.4
Alveolar PCO2 (thick line) and alveolar PO2 (thin line) for Douglas. The other members of the expedition showed similar changes. From Douglas et al [5]
Of course the investigators recognized that the cause of the reduced PCO2 shown in Fig. 16.3 on ascent to altitude was hyperventilation. However they were at a loss to explain the mechanism and there is a somewhat tortuous description of possible reasons such as lactic acid from the hypoxia stimulating the respiratory center, or resetting of the exciting threshold for CO2. Of course they were unaware of the critical role of the peripheral chemoreceptors that were only discovered 15 years later by the two Heymans [19].
16.3 Arterial PO2 and Comparisons with the Alveolar Values
Extensive measurements of the arterial PO2 were made by an indirect technique involving the inhalation of carbon monoxide and then deriving the arterial PO2 from the relation between the hemoglobin bound to oxygen and carbon monoxide. Haldane had developed this method because of his interest in the toxic effects of carbon monoxide in mines. However in the event it was unfortunate that this indirect technique was used because the measurements were erroneous for reasons that are still not fully understood. Another method for measuring the arterial PO2, that is by using an aerotonometer, had been described by the Kroghs [20] and in retrospect this would have been preferable.
The result of the comparisons of alveolar and arterial PO2 on the summit gave an arterial value that averaged about 36 mmHg above the alveolar value and this was interpreted as evidence for oxygen secretion by the lung. Of course this was an error but it should not detract from many other important observations made during the expedition. Haldane actually believed in oxygen secretion throughout his life and indeed a whole chapter of the second edition of his book Respiration [16] published a year before his death was devoted to oxygen secretion. One of the reasons why he took this view was that he was aware that the swim bladder of the fish often contained gas with a much higher PO2 than the surrounding water. He also knew that the swim bladder was a diverticulum of the gastrointestinal tract as was the lung, and so he argued that if the fish could do it, humans could too. In fact Haldane was something of a vitalist and in the introduction to the first edition of Respiration (Haldane, 1921) we read “the mechanistic theory of life is now outworn and must soon take its place in history as a passing phase in the development of biology”. Haldane’s attitudes to vitalism have been discussed elsewhere [22].
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


