Fig. 6.1
Shapes of selected torque-controlled catheters (see text). (a) Pigtail catheter, (b) Amplatz left coronary catheter, (c) Amplatz right coronary catheter, (d) internal mammary catheter, (e) Judkins left coronary catheter catheter, (f) judkins right coronary catheter, (g) multipurpose catheter

Fig. 6.2
Left ventriculography (retrograde approach) with pigtail catheter (Cordis, Miami Lakes, FL) – lateral projection. Multiple ventricular septal defects in a 2-year-old patient after pulmonary artery banding and surgical repair of aortic arch hypoplasia and coarctation
There are angiographic catheters of various curves available in the market. Special shapes have been designed for a variety of purposes, e.g., pulmonary angiography. Despite their different shapes and other features, the main principles remain the same. Therefore, they are not described in this chapter.
Berman angiographic catheter is a balloon-tipped catheter without the end hole (Fig. 6.3a). Thus, it cannot be advanced over a guidewire. Since it has a straight tip, the curved wire can be placed inside the catheter to shape it and support it when entering the desired location. The CO2 inflatable balloon helps to cross the valves with the blood flow. Usually Berman catheter is used to access the right ventricle and the pulmonary arteries (Fig. 6.4). However, in the presence of interatrial or interventricular communications, it can be used to catheterize the left heart structures as well (Fig. 6.5). Antegrade approach to the aorta is feasible also in patients with transposition of the great arteries, double outlet right ventricle, or functionally univentricular hearts or in the presence of large ventricular septal defects. Moreover, the balloon catheter can be used to occlude the distal parts of the vessels and perform occlusion arteriography. Antegrade balloon occlusion aortography with 35° caudal angulation is used to visualize coronary arteries in cases of transposition of the great arteries (Fig. 6.6). Balloon occlusion descending aortography helps to force blood flow through aortopulmonary collateral arteries in the tetralogy of Fallot and other congenital cardiac malformations with pulmonary stenosis or atresia (Fig. 6.7). In fenestrated Fontan patients, one can occlude the fenestration with the balloon tip in order to evaluate changes of blood pressure in the Fontan circulation. All these and many more applications make the Berman angiographic catheter an especially valuable item in the catheterization laboratory inventory.
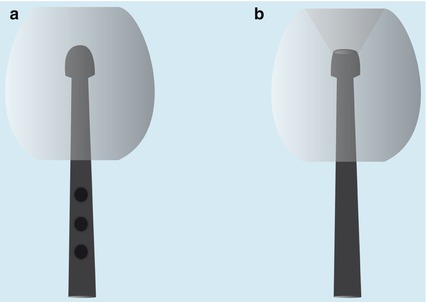
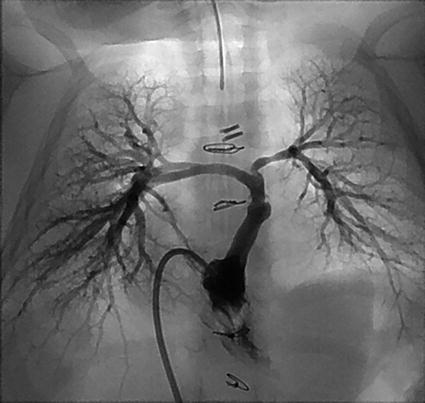

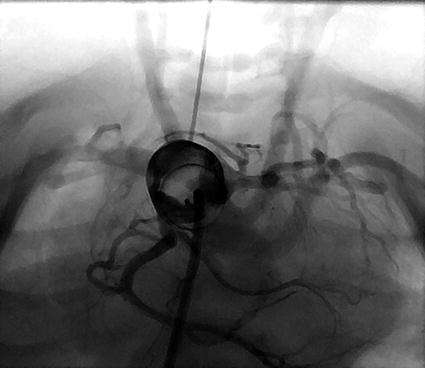
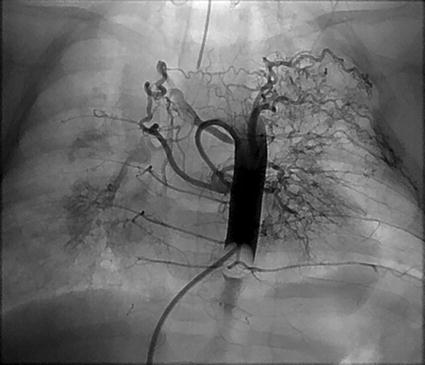
Fig. 6.3
Tips of floating catheters. (a) Berman angiography balloon catheter. (b) Pulmonary wedge balloon catheter
Fig. 6.4
Right ventriculography (antegrade approach) with Berman angiography balloon catheter (Arrow International Inc., Reading, PA) – cranially tilted frontal projection. Patient with hypoplastic right heart syndrome (weight 4 kg) after central shunt due to pulmonary artery hypoplasia
Fig. 6.5
Aortography (antegrade approach) with Berman angiography balloon catheter (Arrow International Inc., Reading, PA) – cranially tilted frontal projection. The patient presented in Fig. 6.4
Fig. 6.6
Balloon occlusion ascending aortography (antegrade approach) with Berman angiography balloon catheter (Arrow International Inc., Reading, PA) – caudally tilted frontal projection. Anatomy of the coronary arteries (origin of the left circumflex artery from the right coronary artery) in a 2-day-old patient with transposition of the great arteries
Fig. 6.7
Balloon occlusion descending aortography (antegrade approach) with Berman angiography catheter (Arrow International Inc., Reading, PA) – posterior-anterior projection. Aortopulmonary collaterals in a 6-month-old patient with double inlet left ventricle after pulmonary artery banding
6.1.2.2 Pulmonary Balloon Wedge Catheters
The pulmonary balloon wedge catheter (Swan-Ganz) is a single end-hole, balloon-tipped catheter, originally invented to measure right heart pressures. Its balloon tip makes it float to the distal pulmonary arteries (Fig. 6.3b). When it reaches the desired position, the inflated balloon occludes the antegrade flow in the vessel. Thus, the pressure in the pulmonary veins and the left atrium can be measured. When placed in the pulmonary vein, one can measure the pressure in the pulmonary arterial bed, based on exactly same principle as the antegrade pulmonary wedge measurement. However, in the hands of interventional cardiologist, the pulmonary balloon wedge catheter becomes more widely used for advancing the guidewire for interventional procedures, selective pulmonary arteriography, simulation of vessel occlusion, and many others. With the balloon inflated at its tip, it should cross the tricuspid valve safely and minimize the risk of its injury during the following interventions: balloon valvuloplasty, pulmonary arteries angioplasty, or stent placement. In case of extreme pulmonary artery hypoplasia, injection of the contrast medium through the catheter wedged in the peripheral pulmonary vein with consecutive flushing with saline results in retrograde visualization of the pulmonary arterial vessels. Antegrade placement of the Swan-Ganz catheter in the Blalock-Taussig shunt is used, after inflation of the balloon, to simulate the shunt occlusion and monitor pressure changes in the pulmonary arteries. Undoubtedly, the pulmonary wedge catheter should always be available for use in the catheterization laboratory shelf.
6.1.2.3 Curved Catheters
A large variety of curved catheters are designed for selective catheterization of blood vessels. As mentioned before, their names often suggest their particular application. However, the interventionist searching for “right ventricular outflow tract catheter” or “right Blalock-Taussig catheter” would be unsuccessful in finding these. The operator should base selection of the most useful equipment on personal preferences, experience of other specialists, knowledge of catheter properties, and the patient’s anatomy. Most of the curved catheters have a single end hole. They can be used for selective angiography, pressure measurement, and guidewire placement.
Selected curved catheters are presented in Fig. 6.1. Some of these, described below, deserve some more attention.
Coronary catheters are designed to easily intubate the normal coronary arteries. Judkins and Amplatz catheters are the most popular (Figs. 6.1b–e, 6.8, 6.9, 6.10, and 6.11). Among them, Judkins right coronary catheter (JR) is one of the most widely used in the cardiac catheterization laboratory. The distal part of the catheter is gently rotated to find support in the ascending aorta and the tip bends at almost a right angle to reach the orifice of the right coronary artery. In pediatric catheterization laboratory, this shape has proved to be useful in the selective catheterization of Blalock-Taussig shunts and collateral vessels (Fig. 6.10). Furthermore, it appears to be the best catheter to enter the right ventricular outflow tract, in cases of extreme pulmonary valve stenosis and pulmonary atresia (Fig. 6.11). In crossing the restrictive interatrial communication in the hypoplastic left heart syndrome, it is worth considering the use of JR catheter inserted over the guidewire to the superior vena cava and gently withdrawing it with the tip directed toward the interatrial septum. Prior to aortic valvuloplasty for neonatal critical aortic stenosis, the JR catheter is the best one for searching the orifice between the stenotic valvar leaflets (Fig. 6.12). JR catheter is also very useful in crossing the interventricular septal defects which is the important step in their interventional closure.
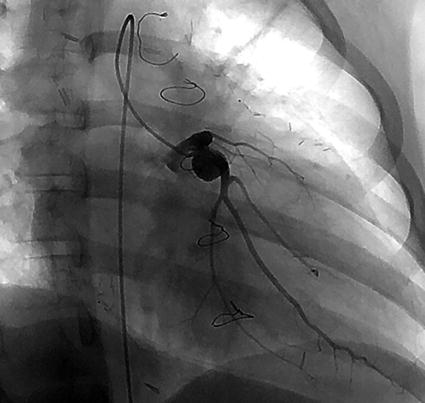
Fig. 6.8
Left coronarography (right anterior oblique projection) with Judkins left coronary catheter (Cordis, Miami Lakes, FL). Details of left coronary artery anatomy (aneurysms, interruption, stenosis) in a 10-year-old patient with Kawasaki disease after bilateral internal mammary arteries/coronary arteries bypass.
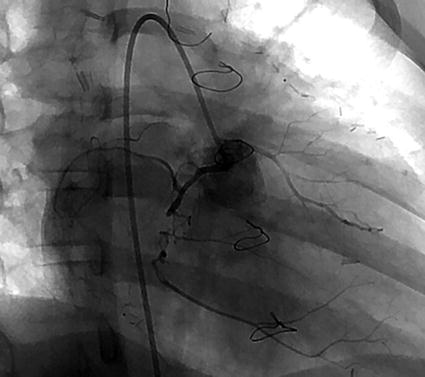
Fig. 6.9
Right coronarography (right anterior oblique projection) with Judkins right coronary catheter (Cordis, Miami Lakes, FL). Details of right coronary artery anatomy (interruption, stenosis) in the patient presented in Fig. 6.8
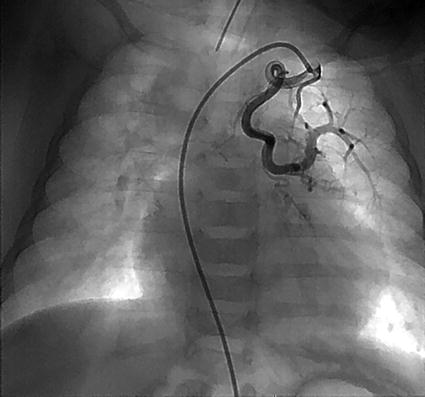
Fig. 6.10
Selective angiography of aortopulmonary collateral artery arising from the left subclavian artery with Judkins right coronary catheter (Cordis, Miami Lakes, FL) – posterior-anterior projection
< div class='tao-gold-member'> Only gold members can continue reading. Log In or Register to continue
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


