Case 6
HISTORY AND PHYSICAL EXAMINATION
An electrodiagnostic (EDX) examination was performed.
Please now review the Nerve Conduction Studies and Needle EMG tables.
QUESTIONS
EDX FINDINGS AND INTERPRETATION OF DATA
Pertinent EDX studies include the following:
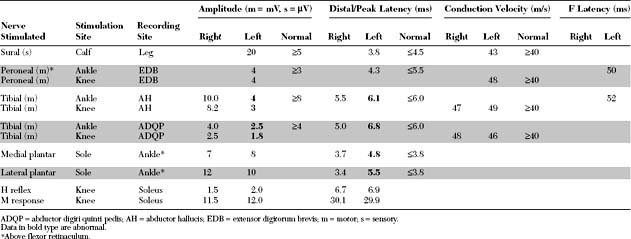
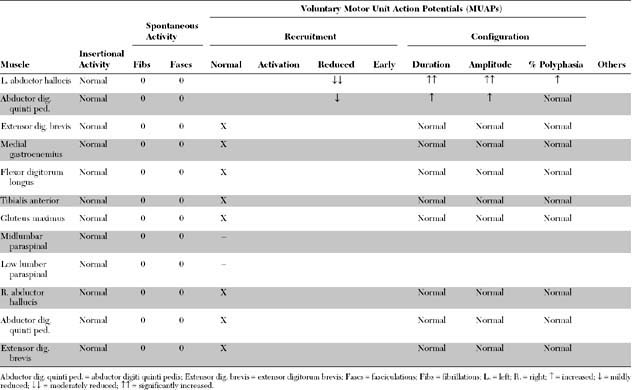
These findings are consistent with a right tibial mononeuropathy at, or distal to, the ankle, affecting both terminal branches (medial and lateral plantar nerves), and compatible with a left tarsal tunnel syndrome (TTS). The study is not consistent with an S1 radiculopathy due to the normal H reflex and lack of denervation in other S1-innervated muscles (medial gastrocnemius, flexor digitorum longus, extensor digitorum brevis, gluteus maximus, and lumbar paraspinal muscles). A sensorimotor polyneuropathy is unlikely because of the lack of denervation in the contralateral foot and normal H reflexes, right sural sensory nerve action potential (SNAP), and left peroneal and right tibial motor distal latencies and conduction velocities.
DISCUSSION
Applied Anatomy
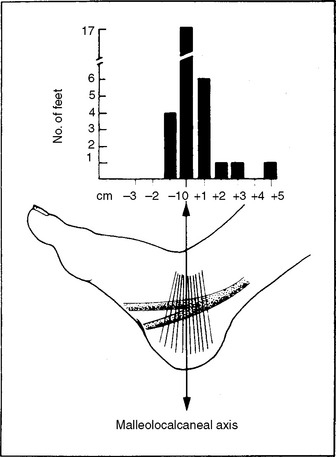
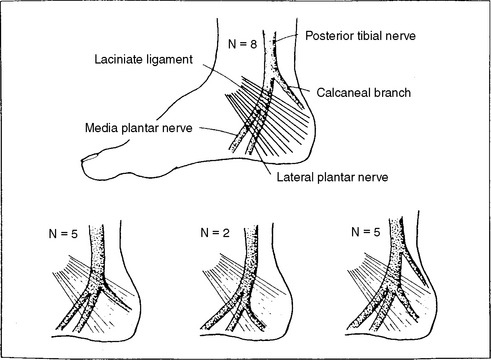
The tibial nerve bifurcates into its two terminal branches within 1 cm of the malleolocalcaneal axis in 90+ of patients (Figure C6-1). Its terminal branches are: (1) the calcaneal branch, a purely sensory nerve, which has a variable takeoff in relation to the flexor retinaculum and explain its involvement or its lack of in nerve entrapments at that site (Figure C6-2); (2) the medial plantar nerve, which innervates the abductor hallucis, flexor digitorum brevis, and flexor hallucis brevis, in addition to the skin of the medial sole and, at least, the medial three toes; and (3) the lateral plantar nerve, which innervates the abductor digiti quinti pedis, flexor digiti quinti pedis, adductor hallucis, and the interossei, in addition to the skin of the lateral sole and two lateral toes. The innervation of the skin of the sole of the foot is provided primarily through the three terminal branches of the tibial nerves, with minimal contribution from the saphenous and sural nerves (Figure C6-3).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


