Case 13
HISTORY AND PHYSICAL EXAMINATION
A cervical spine radiograph showed a rudimentary cervical rib on the right (Figure C13-1). An EMG examination was performed.
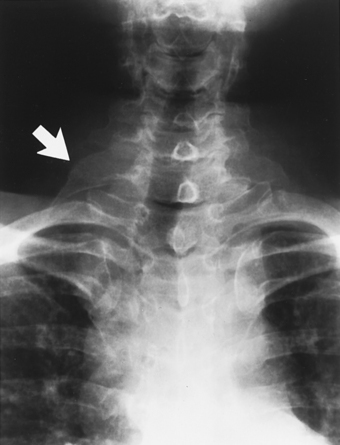
Figure C13-1 The patient’s cervical spine x-ray (anteroposterior view) revealing a rudimentary cervical rib on the right (arrow).
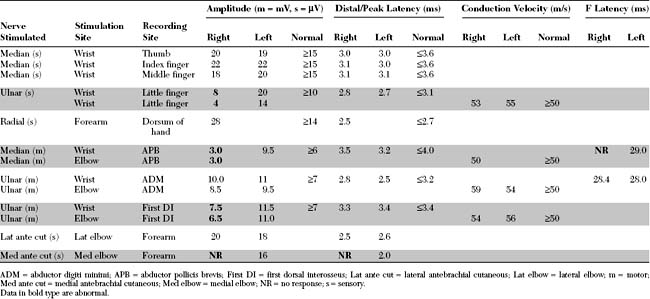
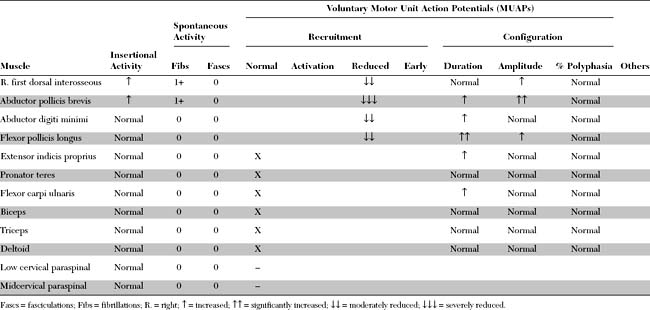
Please now review the Nerve Conduction Studies and Needle EMG tables.
QUESTIONS
EDX FINDINGS AND INTERPRETATION OF DATA
The significant EDX findings in this case include the following:
DISCUSSION
Applied Anatomy
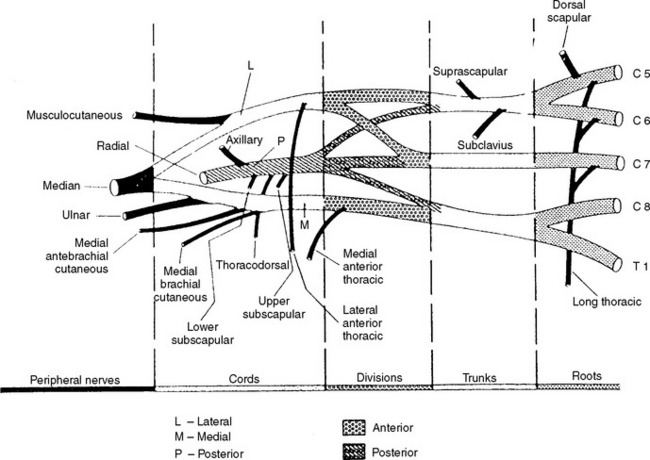
The brachial plexus is derived from the anterior primary rami of the C5 through T1 spinal roots. As is shown in Figure C13-2, these roots intertangle at multiple sites to form structures that usually are divided into five components: roots, trunks, divisions, cords, and peripheral (terminal) nerves. Because the divisions generally are located under the clavicle, some divide the brachial plexus into two regions: supraclavicular (roots and trunks) and infraclavicular (cords and peripheral nerves). Nerve fibers from the C5 and C6 anterior primary rami combine to form the upper trunk, C8 and T1 rami combine to form the lower trunk, and the C7 ramus continues as the middle trunk. Then, each trunk divides into two divisions (anterior and posterior). All three posterior divisions unite to form the posterior cord, the upper two anterior divisions merge to form the lateral cord, and the anterior division of the lower trunk continues as the medial cord.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


