Case 12
HISTORY AND PHYSICAL EXAMINATION
EMG examination was done 5 weeks postinjury.
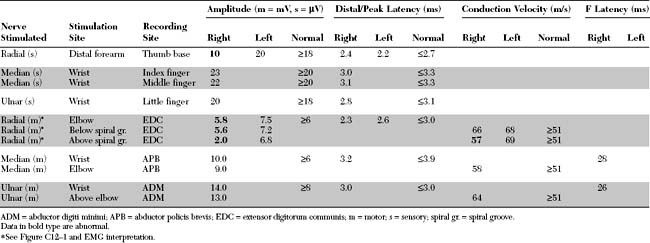
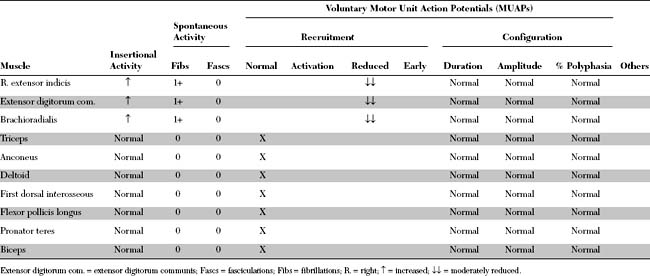
Please now review the Nerve Conduction Studies (NCS) and Needle EMG tables.
QUESTIONS
EDX FINDINGS AND INTERPRETATION OF DATA
Abnormal EDX findings include:
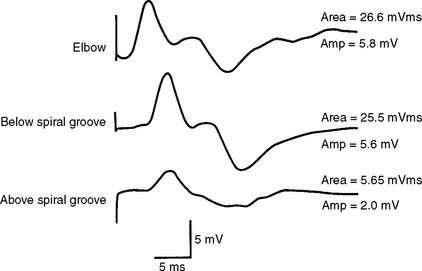
Figure C12-1 Right radial motor conduction studies, recording from the extensor digitorum communis. Note the significant drop in compound muscle action potential (CMAP) amplitude and area during stimulation below compared with above the spiral groove (see also Nerve Conduction table).
DISCUSSION
Applied Anatomy
The radial nerve is the largest nerve in the upper extremity (Figure C12-2). It is a direct extension of the posterior cord of the brachial plexus, after takeoff of the axillary nerve, and contains fibers from all the contributing roots of the plexus (i.e., C5 through T1).
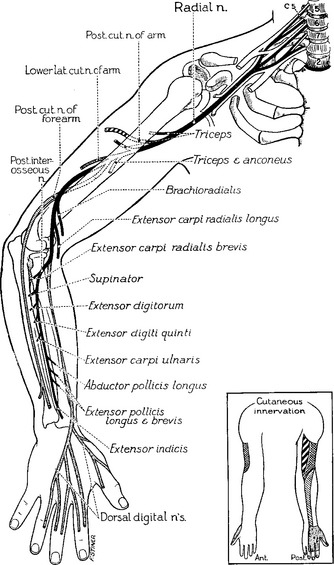
Figure C12-2 Anatomy of the radial nerve and its branches.
(From Haymaker W, Woodhall B. Peripheral nerve injuries: principles of diagnosis. Philadelphia, PA: WB Saunders, 1953, with permission.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


