TABLE 23.1 Assessment of Patency in Vein and Arterial Grafts by MR Angiography Compared with Invasive Angiography | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
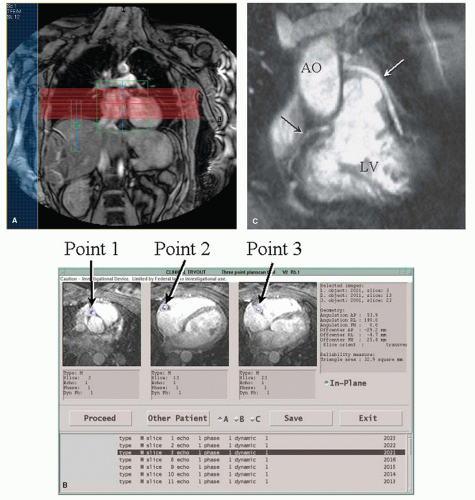 Figure 23.1. Example of a typical MR angiography (MRA) acquisition protocol. A: Typical planscan for coronary MRA. The red lines represent the axial imaging volume, the large green box is the volume used for localized shimming, the rectangular green box is the position in the right hemidiaphragm of the respiratory navigator, and the blue box is the position of a saturation band for suppression of image artifacts. B: Based on axial scout images, the three-point planscan is used to select three points in space, one at the origo of the coronary artery or bypass graft, one at the most distal point, and one in the middle of the first two points. From this information, an imaging plane is automatically calculated in plane with the coronary artery or bypass graft of interest. C: MRA of a patient with a bypass graft to the left coronary system (white arrow) and a visible native right coronary artery (black arrow). This imaging approach can be used clinically to assess bypass graft patency. AO, aorta; LV, left ventricle. |
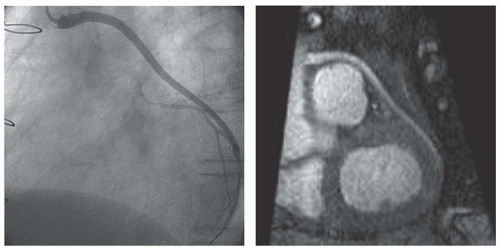 Figure 23.2. Example of an MR angiogram of a vein graft (right panel) in comparison with a coronary angiogram (left panel). A free-breathing, 3D, navigator-gated sequence was used for acquisition, here shown in a multiplanar reformat reconstruction. |
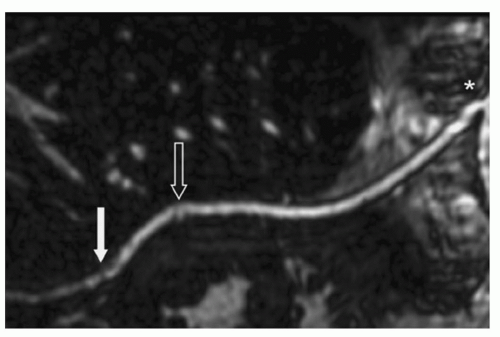 Figure 23.3. 3-T MR angiographic image (curved reconstruction) using an intravascular contrast agent for saphenous vein bypass graft visualization. There is no evidence of stenosis. The bypass graft is patent from the proximal aortic anastomosis (asterisk) to the distal anastomoses with the left coronary artery (arrow: Diagonal artery; open arrow: Marginal artery). (Reproduced with permission from: Hoppe H, Reineke D, Rosskopf AB, et al. Morphological and functional 3-Tesla magnetic resonance imaging of saphenous vein coronary artery bypass grafts. Interact Cardiovasc Thorac Surg. 2011;12:582-585.) |
study adequate biphasic flow profiles could be obtained in 62 of 73 angiographically patent grafts (8). A significant difference in flow between single and sequential grafts to three vascular regions was demonstrated. These early vein graft flow studies were limited by the use of a gradient-echo sequence with limited spatial resolution (1.9 × 1.2 × 5 mm3) and no compensation for respiratory motion on 0.5- to 0.6-T magnets.
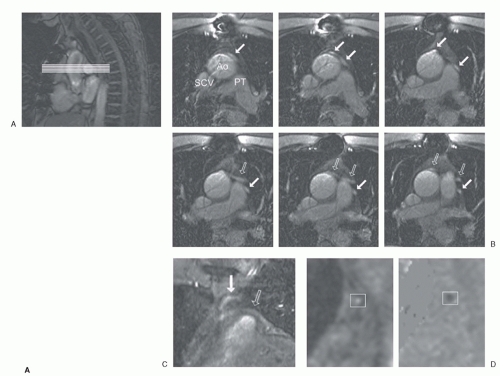 Figure 23.4. Example of an MR flow velocity study. A: Panel A shows a sagittal scout scan, on which the transversal survey scans at the level of the ascending aorta are planned. Panel B depicts the transversal survey scans showing two vein grafts, one to the circumflex region (arrows) and one to the left anterior descending artery (open arrows). Ao, aorta; PT, pulmonary trunk; SCV, supracaval vein. Panel C shows a coronal, oblique survey scan of the two vein grafts. Two differently orientated survey scans are used to plan the flow velocity scan. Panel D illustrates the flow velocity scan (modulus and phase image) in mid-diastole of the first graft at rest, which is used to obtain volume flow. (Reproduced with permission from: Salm LP, Vliegen HW, Langerak SE, et al. Evaluation of saphenous vein coronary artery bypass graft flow by cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2005;7:631-637.) |
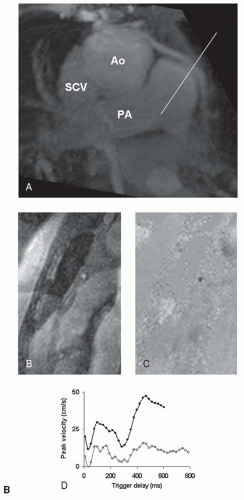 Figure 23.4. (continued) B: One of the survey images is depicted, visualizing a vein graft in plane (Panel A). Panels B and C show the modulus and phase images. The graft is pictured as a white, respectively black spot in the center of the image. In every image in the cardiac cycle 4 pixels in the center of the graft are selected to obtain a velocity curve (Panel D; white dots: Resting curve). The MR flow velocity acquisition is repeated during adenosine-induced stress to obtain the stress velocity curve (black dots). Ao, aorta; PA, pulmonary artery; SCV, supracaval vein. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


