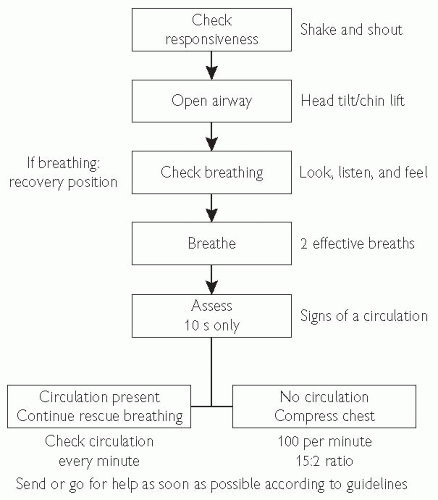
Basic life support (BLS) is the backbone of effective resuscitation following a cardiorespiratory arrest. The aim is to maintain adequate ventilation and circulation until the underlying cause for the arrest can be reversed. 3-4 minutes without adequate perfusion (less if the patient is hypoxic) will lead to irreversible cerebral damage. The usual scenario is an unresponsive patient found by staff, who alert the cardiac arrest team. The initial assessment described below should have already been performed by the person finding the patient. The same person should have also started cardiopulmonary resuscitation (CPR). Occasionally you will be the first to discover the patient, and it is important to rapidly assess the patient and begin CPR. The various stages in basic life support are described here and summarized inFig. 17.1.
1. Assessment of the patient
Ensure safety of rescuer and victim
Check whether the patient is responsive. Gently shake victim and ask loudly ‘are you all right?’
(a) If victim responds, place him/her in the recovery position and get help.
(b) If victim is unresponsive, shout for help and move on to assess airway (see below).
2. Airway assessment
Open the airway. With two fingertips under the point of the chin, tilt the head up. If this fails, place your fingers behind the angles of the lower jaw and apply steady pressure upwards and forwards. Remove ill-fitting dentures and any obvious obstruction. If the patient starts breathing, roll the patient over into the recovery position and try to keep the airway open until an orophyrangeal airway can be inserted.
Keep airway open, look, listen, and feel for breathing. Look for chest movements, listen at the victim’s mouth for breathing sounds and feel for air on your cheek (for no more than 10 seconds).
(a) If patient is breathing, turn them into the recovery position, check for continued breathing and get help.
(b) If patient is not breathing, making occasional gasps, or weak attempts at breathing, send someone (or go for help if alone). (On return) start rescue breaths by giving two slow effective breaths, each resulting in a visible rise and fall in the chest wall.
3. Assessment of circulation
Assess signs of circulation by feeling the carotid pulse for no more than 10 s.
(a) If there are signs of circulation but no breathing, continue rescue breaths and check for signs of breathing every 10 breaths (approximately one breath a minute).
(b) If there are no signs of circulation start chest compression at a rate of 100 times per minute. Combine rescue breaths and compression at the rate of 15 compressions to two effective breaths.
The ratio of compressions to lung inflation remains the same for resuscitation with two persons.
Fig. 17.1 Adult basic life support. For further information see The Resuscitation Council (UK) website http://www.resus.org.uk/.
Adult advanced life support
It is unlikely that an effective spontaneous cardiac activity will be restored by basic life support without more advanced techniques (intubation for effective ventilation, drugs, defibrillation, etc.). Do not waste time. As soon as help arrives, delegate CPR to someone less experienced in advanced cardiac life support (ACLS), so that you are able to continue.
Attach the patient to a cardiac monitor as soon as possible to determine the cardiac rhythm and treat appropriately (see Universal treatment algorithm, p. 716).
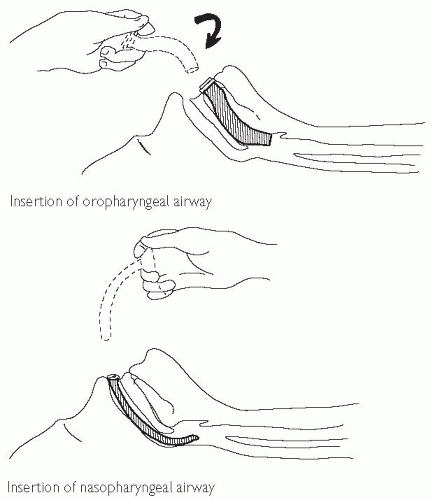
Orophyrangeal (Guedel) or nasopharyngeal airways help maintain the patency of the airway by keeping the tongue out of the way. They can cause vomiting if the patient is not comatose. Endotracheal (ET) intubation is the best method of securing the airway. Do not attempt this if you are inexperienced. See also Figs. 17.2 and 17.3.
Establish venous access. Central vein cannulation (internal jugular or subclavian) is ideal but requires more training and practice, and is not for the inexperienced. If venous access fails, drugs may be given via an ET tube into the lungs (except for bicarbonate and calcium salts). Double the dose of drug if using this route, as absorption is less efficient than IV.
Post-resuscitation care
Try to establish the events that precipitated the arrest from the history, staff, witnesses, and the hospital notes of the patient. Is there an obvious cause (myocardial infarction (MI), hypoxia, hypoglycaemia, stroke, drug overdose or interaction, electrolyte abnormality, etc.)? Record the duration of the arrest in the notes, with the interventions, drugs (and doses) in chronological order.
Examine the patient to check both lung fields are being ventilated; check for ribs that may have broken during CPR. Listen for any cardiac murmurs. Check the neck veins. Examine the abdomen for an aneurysm or signs of peritonism. Insert a urinary catheter. Consider a nasogastric (NG) tube if the patient remains unconscious. Record the Glasgow Coma Score and perform a brief neurological assessment.
Investigations: electrocardiogram (ECG) (looking for MI, ischaemia, tall T waves (↑K+)); arterial blood gases (ABG) (mixed metabolic and respiratory acidosis is common and usually responds to adequate oxygenation and ventilation once the circulation is restored; if severe, consider bicarbonate); chest X-ray (CXR; check position of ET tube, look for pneumothorax); urea and electrolytes (U&Es), and glucose.
After early and successful resuscitation from a primary cardiac arrest, the patient may rapidly recover completely. The patient must be transferred to high-dependency unit (HDU) or coronary care unit (CCU) to monitor for 12-24 h. Commonly the patient is unconscious post-arrest and should be transferred to the intensive therapy unit (ITU) for mechanical ventilation and haemodynamic monitoring and support for ≥ 24 hours.
Change any venous lines that were inserted at the time of arrest for central lines inserted with sterile technique. Insert an arterial line and consider a pulmonary artery (PA) catheter (Swan-Ganz) if requiring inotropes.
Remember to talk to the relatives. Keep them informed of events and give a realistic (if bleak) picture of the arrest and possible outcomes.
When appropriate, consider the possibility of organ donation and do not be frightened to discuss this with the relatives. Even if discussion with the relatives is delayed, remember corneas and heart valves may be used up to 24 hours after death.
Fig. 17.2 Opening airways. Reproduced with permission from Ramrakha P, Moore K, Sam M (2010). Oxford Handbook of Acute Medicine, 3rd ed. Oxford: Oxford University Press.
Fig. 17.3 Insertion of nasopharyngeal airway. Reproduced with permission from Ramrakha P, Moore K, Sam M (2010). Oxford Handbook of Acute Medicine, 3rd ed. Oxford: Oxford University Press.
Universal treatment algorithm
Cardiac rhythms of cardiac arrest can be divided into two groups:
2. other cardiac rhythms, which include asystole and pulseless electrical activity (PEA).
The principal difference in treatment of the two groups of arrhythmias is the need for attempted defibrillation in the VF/VT group of patients.
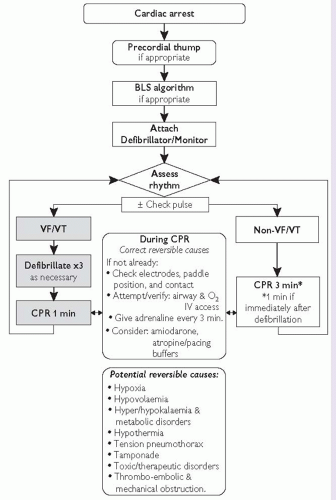
Fig. 17.4 summarizes the algorithm for management of both groups of patients.
VF/VT
VF/VT are the most common rhythms at the time of cardiac arrest.
Success in treatment of VF/VT is dependent on the delivery of prompt defibrillation. With each minute, the chances of successful defibrillation decline by 7-10%.
Precordial thump: if arrest is witnessed or monitored, a sharp blow with a closed fist on the patient’s sternum may convert VF/VT back to a perfusing rhythm. It is particularly effective if delivered within 30 s after cardiac arrest.
Shock cycles are generally in groups of three. Initially 200 J, 200 J, and 360 J, with subsequent cycles at 360 J.
After each shock (or sequence), the carotid pulse should be palpated only if the waveform changes to one usually capable of providing a cardiac output.
The shock cycle is repeated every minute if VF/VT persists.
Myocardial and cerebral viability must be maintained after each shock cycle, with chest compressions and ventilation.
In between cycles of defibrillation, reversible factors must be identified and corrected, the patient intubated (if possible) and venous access obtained.
Adrenaline should be given every 3 minutes (1 mg IV and 2-3 mg via endotracheal route).
Non-VF/VT rhythms
The outcome from these rhythms is generally worse than VF/VT unless a reversible cause can be identified and treated promptly.
Chest compressions and ventilation should be undertaken for three minutes with each loop of the algorithm (1 min if directly after a shock).
With each cycle, attempts must be made to intubate the patient, gain IV access and give adrenaline.
Asystole
Atropine 3 mg IV should be given to block all vagal output.
In the presence of P waves on the ECG strip/monitor, pacing (external or transvenous) must be considered.
PEA
Identification of the underlying cause and its correction are both vital for successful resuscitation. Resuscitation must be continued while reversible causes are being sought.
Fig. 17.4 The advanced life support universal algorithm for the management of cardiac arrest in adults. For further information see The Resuscitation Council (UK) website http://www.resus.org.uk/.
Primary percutaneous coronary intervention for acute ST-segment elevation myocardial infarction (see p. 268)
Primary percutaneous coronary intervention (PCI) is the current gold standard reperfusion strategy for treatment of ST-segment elevation MI (STEMI).
Primary PCI requires significant coordination between the emergency services, community hospitals, and invasive centres. It must only be performed if: (1) a primary PCI programme is available; (2) the patient presents to an invasive centre and can undergo catheterization without delay.
Indication for primary PCI
All patients with chest pain and ST-segment elevation or new left bundle branch block (LBBB) fulfil primary PCI criteria (compare with indications for thrombolysis).
This will include a group of patients where ST-segment elevation may not fulfil thrombolysis criteria.
In general, patients in whom thrombolysis is contraindicated should be managed by primary PCI. Cases where there is significant risk of bleeding must be managed individually.
chest pain or palpitations—? ischaemic heart disease (IHD)/MI, arrhythmia
preceding history of dyspnoea on exertion—? IHD, poor left ventricular (LV) function
oliguria, haematuria—? acute renal failure
seizures, signs of intracranial bleed.
Causes
A diagnosis of pulmonary ooedema or ‘heart failure’ is not adequate. An underlying cause must be sought in order to direct treatment appropriately. Causes may be divided into:
Often there is a combination of factors involved (e.g. pneumonia, hypoxia, cardiac ischaemia); see Drugs for hypertensive emergencies, p. 760.
The main differential diagnosis is acute (infective) exacerbation of chronic obstructive pulmonary disease (COPD) (previous history, quiet breath sounds ± wheeze, fewer crackles). It may be difficult to differentiate the two clinically.
Principles of management
Stabilize the patient—relieve distress and begin definitive treatment.
Look for an underlying cause.
Address haemodynamic and respiratory issues.
Optimize and introduce long-term therapy.
Initial rapid assessment
If the patient is very unwell (e.g. unable to speak, hypoxic, systolic BP <100 mmHg), introduce stabilizing measures and begin treatment immediately before detailed examination and investigations (see Pulmonary oedema: management, p. 728).
If the patient is stable and/or if there is doubt as to the diagnosis, give oxygen and diuretic, but await the outcome of clinical examination and CXR before deciding on definitive treatment.
To confirm the diagnosis, looking for interstitial shadowing, enlarged hila, prominent upper lobe vessels, pleural effusion, and Kerley B lines. Cardiomegaly may or may not be present. Also exclude pneumothorax, pulmonary embolus (oligaemic lung fields), and consolidation
Typically ↓PaO2. PaCO2 levels may be ↓ (hyperventilation) or ↑ depending on the severity of pulmonary oedema. Pulse oximetry may be inaccurate if peripherally shut down
U&Es
? pre-existing renal impairment. Regular K+ measurements (once on IV diuretics)
Note: the critical LA pressure for hydrostatic ooedema = serum albumin (g/L) x 0.57.
Pulmonary oedema: management
Stabilize the patient
Patients with acute pulmonary oedema should initially be continuously monitored and managed where full resuscitation facilities are available.
Sit the patient up in bed.
Give 60-100% oxygen by face mask (unless contraindicated, COPD).
If the patient is severely distressed, summon the ‘on-call’ anaesthetist and inform ITU. If dyspnoea cannot be significantly improved by acute measures (below) the patient may require continuous positive airways pressure (CPAP) or mechanical ventilation.
Treat any haemodynamically unstable arrhythmia (urgent synchronized DC shock may be required (see DC cardioversion, p. 818).
If the systolic blood pressure is ≥90 mmHg and the patient does not have aortic stenosis:
give sublingual glyceryl trinitrate (GTN) spray (2 puffs)
start IVGTN infusion 1-10 mg/h, increase the infusion rate every 15-20 minutes, titrating against blood pressure (aiming to keep systolic BP ˜100 mmHg).
If the systolic blood pressure is <90 mmHg, treat patient as cardiogenic shock (see NSTEMI/UA: invasive versus non-invasive strategies, p. 301).
Insert a urinary catheter to monitor urine output.
Repeat ABG and K+ if the clinical condition deteriorates/fails to improve, or after 2 h if there is improvement and the original sample was abnormal.
Monitor pulse, BP, respiratory rate, O2 saturation with a pulse oximeter (if an accurate reading can be obtained), and urine output.
If the patient responds arrange appropriate investigations as listed on Acute pulmonary oedema: assessment, p. 724 to help with further management. However, if there is further deterioration, specific measures should be taken to address problems.
Further management
The subsequent management of the patient is aimed at ensuring adequate ventilation/gas exchange and haemodynamic stability and correcting any reversible precipitins of acute pulmonary oedema.
Assess the patient’s respiratory function:
does the patient require respiratory support?
Assess the patient’s haemodynamic status (see Cardiogenic shock, p. 288):
is the patient in shock (?(see Cardiogenic shock, p. 288).
Look for an underlying cause (see Pulmonary oedema: causes, p. 726).
If the patient remains unstable and/or deteriorates, assess their respiratory function.
Assessment of respiratory function
Wheeze may be caused by interstitial pulmonary oedema. If there is a history of asthma, give nebulized salbutamol (2.5-5 mg), nebulized ipratropium bromide (500 mcg), and hydrocortisone (200 mg) IV. Consider commencing aminophylline infusion. This will relieve bronchospasm, as well as ‘off-load’ by systemic vasodilatation. However, it may worsen tachycardia, and can be arrhythmogenic and lower K+ (supplement to ensure K+ 4-5 mmol/L).
Indications for further respiratory support include:
patient exhaustion or continuing severe breathlessness
CPAP: this may be tried for co-operative patients, who can protect their airway, and have adequate respiratory muscle strength and who are not hypotensive. The positive pressure reduces venous return to the heart and may compromise BP.
Endotracheal intubation and mechanical ventilation may be required, and some positive end-expiratory pressure (PEEP) should be used.
Discuss the patient with the on-call anaesthetist or ITU team early.
Assess the patient’s haemodynamic status
It is important to distinguish between cardiogenic and non-cardiogenic pulmonary oedema, as further treatment is different between the two groups. This may be difficult clinically. A PA (Swan-Ganz) catheter must be inserted if the patient’s condition will allow.
Non-cardiogenic pulmonary oedema occurs when the hydrostatic pressure within the capillary system exceeds the plasma oncotic pressure. In patients with hypoalbuminaemia this will occur at a pulmonary capillary wedge pressure (PCWP)<15 mmHg. The critical PCWP may be estimated by serum albumin (g/L) x 0.57. Thus, a patient with a serum albumin of 15 g/L will develop hydrostatic pulmonary oedema at a LA pressure of 8 mmHg; a serum albumin of 30 g/L will require an LA pressure of > 17 mmHg, and so on …
Cardiogenic pulmonary oedema is often associated with significant systemic hypotension or low-output states. Contributing factors include conditions where there is ‘mechanical’ impairment to forward flow (e.g. valvular heart disease (especially if acute), VSD), or severe myocardial disease (large MI, ongoing ischaemia, acute myocarditis, cardiomyopathy).
The gradient between PA diastolic pressure (PAD) and PCWP (PAD – PCWP) is generally <5 mmHg in cardiogenic and > 5 mmHg in non-cardiogenic pulmonary oedema (e.g. ARDS).
The pulse and BP are most commonly elevated due to circulating catecholamines and overactivity of the renin-angiotensin system (RAS). Examination reveals sweating, cool ‘shut-down’ peripheries, high pulse volume (assess carotid or femoral pulses).
Management
The general approach involves combination of diuretics, vasodilators ± inotropes. Patients may be divided into two groups:
patients in shock (with systolic BP<100 mmHg)—see Pulmonary oedema: management, p. 728
haemodynamically stable patients with systolic BP > 100 mmHg— (see Pulmonary oedema, p. 726-733.
Patients with systolic BP<100 mmHg
The patient is in incipient (or overt) shock. The most common aetiology is cardiogenic shock but remember non-cardiogenic causes (e.g. ARDS, septic shock).
Optimal monitoring and access: central line ±PA catheter (Swan-Ganz), urinary catheter, arterial line (monitoring BP and ABG). Internal jugular lines are preferable, as the risk of pneumothorax is lower.
Ensure the patient is not underfilled, using PCWP as a guide (<10 mmHg) (mistaken diagnosis e.g. septic shock from bilateral pneumonia).
Is there a mechanical cause that may require emergency surgery?
VSD and acute mitral regurgitation (MR) in all patients with recent MI with/without new murmur (see Ventricular septal defect post-MI, p.278; Acute mitral regurgitation post-MI, p.280)
prosthetic heart valve dysfunction (e.g. dehiscence, infection) or pre-existing native aortic or mitral disease that may require surgery.
Discuss the patient early on with cardiologist/cardiac surgeon.
The choice of inotropic agent depends on the clinical condition of the patient and, to some extent, the underlying diagnosis:
Systolic BP 80-100 mmHg and cool peripheries: start dobutamine infusion at 5 mcg/kg/min, increasing by 2.5 mcg/kg/min every 10-15 minutes to a maximum of 20 µg/kg/min until BP > 100 mmHg. This may be combined with dopamine (2.5-5 mcg/kg/min). However, tachycardia and/or hypotension secondary to peripheral vasodilation my limit its effectiveness. Phosphodiesterase inhibitors (enoximone or milrinone) should be considered where dobutamine fails.
Only gold members can continue reading. Log In or Register to continue
 http://www.resus.org.uk/.
http://www.resus.org.uk/. Universal treatment algorithm, p. 716).
Universal treatment algorithm, p. 716).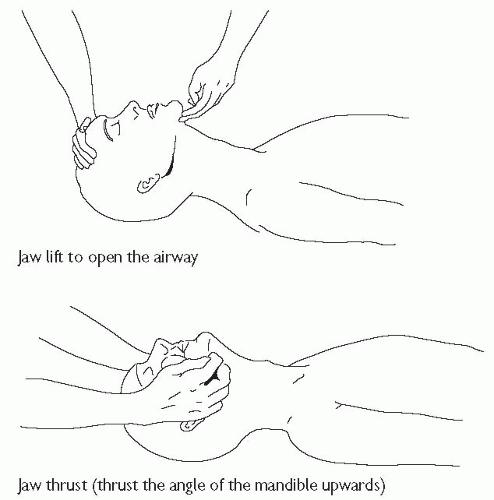
 http://www.resus.org.uk/.
http://www.resus.org.uk/. p. 268)
p. 268)




















 p. 494
p. 494 p. 498)
p. 498) p. 498)
p. 498) p. 508)
p. 508) Drugs for hypertensive emergencies, p. 760.
Drugs for hypertensive emergencies, p. 760. Pulmonary oedema: management, p. 728).
Pulmonary oedema: management, p. 728). DC cardioversion, p. 818).
DC cardioversion, p. 818). NSTEMI/UA: invasive versus non-invasive strategies, p. 301).
NSTEMI/UA: invasive versus non-invasive strategies, p. 301). Acute pulmonary oedema: assessment, p. 724 to help with further management. However, if there is further deterioration, specific measures should be taken to address problems.
Acute pulmonary oedema: assessment, p. 724 to help with further management. However, if there is further deterioration, specific measures should be taken to address problems. Cardiogenic shock, p. 288):
Cardiogenic shock, p. 288): Cardiogenic shock, p. 288).
Cardiogenic shock, p. 288). Pulmonary oedema: causes, p. 726).
Pulmonary oedema: causes, p. 726).

 Ventricular septal defect post-MI, p.278; Acute mitral regurgitation post-MI, p.280)
Ventricular septal defect post-MI, p.278; Acute mitral regurgitation post-MI, p.280)



