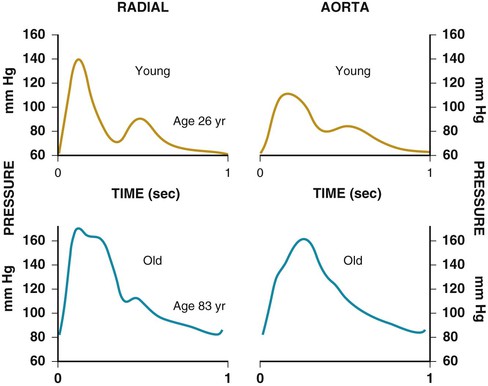
Janice B. Schwartz, Douglas P. Zipes The proportion of people aged 65 years and older in the United States is projected to increase from 12.4% (35 million) of the population in 2000 to 19.6% (71 million) by 2030, with 82 million in that age group by 2050. The number of people older than 80 years of age is projected to double from 9.3 million in 2000 to 19.5 million in 2030, and to more than triple by 2050. Women represented 59% of persons aged older than 65 years in 2000 and have been estimated to constitute 56% of the older population by 20301 (Fig. 76-1). Global trends are similar, with the worldwide population older than 65 years projected to increase to 973 million, or 12%, in 2030 and to constitute approximately 20% of the population in 2050. (See also Chapters 1 and 2; additional epidemiologic and demographic data are available from the Centers for Disease Control and Prevention [www.cdc.gov].) Cardiovascular disease is both the most frequent diagnosis and the leading cause of death among both men and women older than 65 years. Hypertension occurs in one half to two thirds of people older than 65 years, and heart failure (HF) is the most frequent hospital discharge diagnosis among older Americans. The profile of these common cardiovascular diseases differs in older patients from that in younger patients. Systolic but not diastolic blood pressure increases with aging, resulting in increased pulse pressure. Systolic hypertension becomes a stronger predictor of cardiovascular events, especially in women (see Chapter 43). HF with preserved ejection fraction becomes more common at older ages and is more common in women (see Chapter 27). Coronary artery disease (CAD) is more likely to involve multiple vessels and to affect the left main artery and occurs with similar frequency in women and in men older than 65 years. Equal numbers of older men and women present with acute myocardial infarction (MI) until the age of 80 years, after which this presentation is more common in women. Non–ST-segment rather than ST-segment elevation MI accounts for two thirds of the cases in older patients (see Chapters 51 to 54). Diagnosis of stroke is made in 20% to 25% of patients after the age of 80 years (see Chapter 59). More than 80% of all deaths attributable to cardiovascular disease occur in people older than 65 years, with approximately 60% of deaths in those older than 75 years. An important point is that cardiovascular disease in older people is not seen in isolation. Eighty percent of older Americans have at least one chronic medical condition, and half have at least two. Arthritis affects approximately 60% of persons older than 65 years, cancer is present in 34%, and diabetes affects approximately 20% (Fig. 76-2). It is not as well recognized that changes in the prevalence of these diseases occur with aging from 65 to 100 years. In particular, diabetes prevalence decreases, whereas anemia, arthritis, cancer, and dementia increase in prevalence. Dementia that impairs memory, decision-making ability, orientation to physical surroundings, and language is estimated to be present in 13% of community-dwelling white persons older than 65 years and is more prevalent in women than in men and African-American and Hispanic populations.2 By the age of 80, approximately 40% of people may be affected. The high morbidity and mortality from cardiovascular disease in the elderly population warrant aggressive approaches to prevention and treatment that are effective in older patients. Compelling data demonstrate reduced morbidity and mortality rates for the treatment of hypertension, HF with reduced ejection fraction, atrial fibrillation, acute coronary syndromes, CAD, stroke, diabetes, and lipid abnormalities in older patients 60 to 74 years of age, although data on minorities and women are limited. Fewer trials of cardiovascular therapies have enrolled significant numbers of men or women older than 75 years, elderly patients with multisystem disease, or elderly patients with cognitive impairment, and none have addressed cardiovascular therapies in the nursing home population. When clinical trials enroll older patients, participants differ markedly from the most older patients. The projected increase in numbers of older people from previously understudied and undertreated groups presents both medical and economic challenges for cardiovascular disease treatment. No universal definition of “elderly” has been recognized, nor has an accurate biomarker for aging been identified. Although physiologic changes associated with aging do not appear at a specific age and do not proceed at the same pace in all people, most definitions are based on chronologic age. The World Health Organization uses 60 years of age to define “elderly,” whereas most U.S. classifications use the age of 65 years. Gerontologists subclassify the older population into three age groups: young old (60 to 74 years), old old (75 to 85 years), and very old (older than 85 years of age). Cardiovascular society statements have addressed differences in responses between patients older than 65 years, those 65 to 74 years, and those 75 to 84 years of age separately from those older than 85 years of age. Clinicians often separate older patients into two subgroups—those 65 to 80 years of age and those older than 80 years, to highlight the frailty, reduced capacity (physical and mental), and presence of multiple disorders that are more common after the age of 80. Hallmarks of cardiovascular aging include progressive increases in systolic blood pressure, pulse pressure, pulse wave velocity, and left ventricular (LV) mass and increased incidence of CAD and atrial fibrillation.3,4 Reproducible age-related decreases are seen in rate of early LV diastolic filling, maximal heart rate, maximal cardiac output, maximum aerobic capacity or maximal oxygen consumption (VO2max), exercise-induced augmentation of ejection fraction, reflex response of heart rate, heart rate variability, and vasodilation in response to beta-adrenergic stimuli or endothelium-mediated vasodilator compounds. Cellular, enzymatic, and molecular alterations in the arterial vessel wall include migration of activated vascular smooth muscle cells into the intima, with increased matrix production resulting from altered activity of matrix metalloproteinases, angiotensin II, transforming growth factor beta (TGF-β), and intercellular cell adhesion molecules and production of collagen and collagen cross-linking. Also seen are loss of elastic fibers, increases in fibronectin, and calcification. These processes lead to arterial dilation and increased intimal thickness, resulting in increased vascular stiffness. Increased arterial stiffness is manifested by increases in pulse-wave velocity away from the heart and increased and earlier pulse wave reflections back toward the heart (often estimated as the aortic augmentation index). Typical central aortic and radial waveforms from a young and an older person are shown in Figure 76-3. In both animal and human models of aging, endothelial cell production of nitric oxide (NO) decreases with age; additional changes are decreased endothelial cell mass associated with increased cell senescence and apoptosis and increased NO consumption caused by age-dependent increases in vascular superoxide anion production. These changes contribute to reduced endothelial cell NO-mediated vasodilatory responses of the peripheral and coronary vasculature. Vascular responses to beta-adrenergic agonists and alpha-adrenergic blockade also are reduced with aging. By contrast, responses to non–endothelial cell–derived compounds such as nitrates or nitroprusside are preserved with aging but may vary by vascular bed or be altered in diseases such as hypertension or diabetes. Changes in the extracellular matrix of the myocardium parallel those in the vasculature, with increased collagen, increased fibril diameter and collagen cross-linking, an increase in the ratio of type I to type III collagen, decreased elastin content, and an increase in fibronectin. There may also be a shift in the balance between matrix metalloproteinases and tissue inhibitors of matrix metalloproteinases that favor increased production of extracellular matrix. Fibroblast proliferation is induced by growth factors—in particular, angiotensin-transforming growth factors, tumor necrosis factor alpha (TNF-α), and platelet-derived growth factor. These changes are accompanied by cell loss and altered cellular function. In the atria, decreased sinus node cells, decreased L-type calcium channels within sinus node cells, and extracellular matrix changes contribute to sinus node dysfunction and atrial fibrillation. Collagen, elastic tissue, and calcification changes in or near the central fibrous body and the atrioventricular node or proximal bundle branches contribute to conduction abnormalities and annular valvular calcification. In the ventricle, collagen deposition and extracellular matrix changes contribute to loss of cells and hypertrophy of myocytes with changes in myosin subforms and altered myocardial calcium handling.4 Changes in myocardial calcium handling include reduced or delayed inactivation of L-type transmembrane calcium current, decreased and delayed intracellular ionized calcium uptake by cardiac myocyte sarcoplasmic reticulum, and reduced and delayed outwardly directed potassium rectifier current activation. The result is prolongation of the membrane action potential and inward calcium current with prolongation of both contraction and relaxation. Age-related changes also are seen in the intravascular environment. Increases in fibrinogen, coagulation factors V, VIII and IX, and XIIa, and von Willebrand factor are seen without countering increases in anticoagulant factors (see Chapter 82). Platelet phospholipid content is altered and platelet activity is increased, with increased binding of platelet-derived growth factor to the arterial wall, in older compared with younger persons. Increased levels of plasminogen activator inhibitor type 1 (PAI-1) are seen with aging, especially during stress, resulting in impaired fibrinolysis. Circulating prothrombotic inflammatory cytokines, especially interleukin-6, also increase with age and may play a role in the pathogenesis of acute coronary syndromes. All of these changes also potentiate development of atherosclerosis.4 Consistent changes in the autonomic nervous system accompany aging and influence cardiovascular function (see Chapter 89). For the beta-adrenergic system, age-related changes include decreased receptor numbers, altered G protein coupling, and altered G protein–mediated signal transduction. Age-related decreases in alpha-adrenergic platelet receptors and decreased alpha-adrenergic–mediated arterial vasoreactivity of forearm blood vessels occur, whereas alpha-adrenergic–mediated changes in human hand veins appear to be preserved. Dopaminergic receptor content and dopaminergic transporters decrease, and cardiac contractile responses to dopaminergic stimulation may be blunted with aging. Decreased sensitivity and responses to parasympathetic stimulation are seen in cardiac and vascular tissues, whereas increased central nervous system effects frequently are seen in aging models. The combined age-related autonomic changes lead to decreased baroreflex function and responses to physiologic stressors with increased sensitivity to parasympathetic stimulation of the central nervous system. Unifying hypotheses for age-related changes throughout the body include cumulative oxidative damage, inflammatory responses to cellular stress or infection, and programmed cell death. Some age-related cardiovascular changes can be partially, if not totally, reversed by exercise. Exercise improves endothelial function, measures of arterial stiffness, and baroreceptor function in older people. Caloric restriction slows aging and cardiac changes as well as increasing maximal lifespan in several small animal models but has failed to increase longevity in rhesus monkeys. In humans, caloric restriction decreases weight and blood pressure and modifies risk factors for atherosclerosis and can improve indices of diastolic function in short-term experiments, safety and feasibility studies for longer-term studies are under way. Medications such as angiotensin-converting enzyme (ACE) inhibitors, aldosterone antagonists, or beta blockers may influence vascular and cardiac remodeling associated with hypertension, atherosclerosis, or HF.4 Pilot studies suggest that combined exercise, stress management, and specialized diet to lower LDL also increase telomerase activity, and that cellular aging processes can be slowed.5 Dietary antioxidant intake has been associated with slowing of age-related changes in the vasculature but pharmacologic approaches with anti-inflammatory and antioxidant vitamin administration and lowering of homocysteine with B vitamins or omega-3 free fatty acids for either primary or secondary prevention have not been successful in humans. Similarly, dehydroepiandrosterone has not been shown to have significant beneficial effects in older women or men. The most recent vitamin to be targeted for study is vitamin D. Decreased nutritional intake of vitamin D and sun exposure has resulted in vitamin D deficiency in high proportions of Americans, especially the elderly. A large study of vitamin D supplementation in older men and women to determine effects on cardiovascular events and cancer occurrence is under way. Other potential antiaging agents under investigation include those that directly target advanced glycation end products, inflammation, and collagen cross-links. Age-related changes create a cardiovascular system subject to increased pulsatile load and one that is less able to increase output in response to stress. Such changes also limit maximal capacity and decrease reserve capacity, contributing to lower thresholds for symptoms in the presence of cardiovascular diseases that become more common with increasing age. Table 76-1 summarizes age-related cardiovascular changes contrasted with cardiovascular disease. The vast majority of therapeutic interventions for elderly patients are pharmacologic, making appropriate drug selection and modification of dosing regimens for this population important (see Chapter 9). On average, body size decreases with aging, and body composition changes result in decreased total body water, intravascular volume, and muscle mass. Age-related changes are continuous but are most pronounced after the age of 75 to 80 years. Women, with the exception of African American women, tend to weigh less and have smaller intravascular volumes and muscle mass than men at all ages (Fig. 76-4). Higher serum concentrations of medications will be found in older patients, and especially older white and Asian women, if initial doses are the same as in younger patients. Weight adjustments for loading doses of the cardiovascular drugs digoxin and type I and type III antiarrhythmic drugs, aminoglycoside antibiotics, chemotherapy regimens, and unfractionated heparin are standard (see Chapter 7). When fibrinolytic drugs have been administered without weight-based dosage adjustments, increased risk of intracranial hemorrhage has been documented in older, smaller, and female patients.6 Bleeding associated with low-molecular-weight heparins in combination with other lytic agents can be reduced by using weight-based dosing. Routine weight-based adjustments should be made in loading doses of medications, especially those with a narrow therapeutic index. The result usually is a lower loading dose in older patients than in younger patients, with the lowest doses in older white and Asian women. Chronic Medication Administration Renal clearance (see Chapter 88) by all routes—glomerular filtration and renal tubular reabsorption and secretion—decreases with age and is lower in women than in men at all ages. Considerable intersubject variability is recognized, but a general estimate is a 10% decline in glomerular filtration rate (GFR) per decade, with 15% to 25% lower rates in women than in men. The Cockcroft and Gault (C&G) algorithm to estimate creatinine clearance includes age, sex, weight, and serum creatinine concentration as variables: and highlights that significant decreases in renal elimination can be present in older patients with normal serum creatinine levels. With elevations of serum creatinine, severe renal impairment is likely. The Modification of Diet in Renal Disease Study (MDRD) algorithm incorporates creatinine, age, race, and sex as variables nonlinearly and is widely reported by clinical laboratories.8 The MDRD equation for estimated glomerular filtration rate (eGFR) is For SI units: eGFR = (3.1 × (Serum Cr µmol/L/88.4)−1.154 × Age−0.203 × Sex × Race Recently, the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) developed an algorithm (see below) that uses the same four variables but is more accurate in the higher ranges of GFR and classifies fewer people as having renal disease.9 The National Kidney Foundation recommends that the CKD-EPI equation replace the MDRD algorithm for clinical use. Little to no difference between estimates with the two algorithms was seen for people older than 75 years of age when directly compared in a large community sample.10 The CKD-EPI formula is where k = 0.7 for women and 0.9 for men, α = −0.329 for women and −0.411 for men, min indicates the minimum of (Serum Cr/k or 1), and max indicates the maximum of (Serum Cr/k or 1). Addition of cystatin(Cys) C in the CKD-EPI equation reduces bias at eGFR greater than 60, and the most accurate estimation algorithm is the combined creatinine-cystatin C equation that has not yet been incorporated into routine clinical use.10a The CKD-EPI equation is: where κ = 0.7 for women and 0.9 for men, α = −0.248 for women and −0.207 for men, min indicates the minimum of Serum Cr/κ or 1, and max indicates the maximum of Serum Cr/κ or 1. Online and downloadable creatinine clearance and eGFR calculators are available on the National Kidney Foundation website (http://www.kidney.org). The C&G formula predicts a linear decrease with age that is steeper than predicted from the nonlinear decline determined using the MDRD or CKD-EPI eGFR formulas (see Fig. 76-5). Estimates are thus lower with C&G formula compared with MDRD or CKD-EPI. U.S. Food and Drug Administration (FDA)-approved package labeling and most guidelines make dose adjustment recommendations based on estimated creatinine clearance (C&G formula) to reduce excess dosing, whereas MDRD and CKD-EPI GFR estimates are used to classify renal status, risk of procedures and renal complications. All algorithms predict an “average” white woman older than 65 years with a serum creatinine of 1 (average for age 65 years in the National Health and Nutrition Examination Survey [NHANES]) to have stage 3 renal function (http://www.kidney.org) or moderate renal failure (see Fig. 76-5). Failure to adjust dosages of renally cleared medications with a narrow therapeutic index such as thrombolytic agents, low-molecular-weight heparin, and glycoprotein (GP) IIb/IIIa inhibitors has resulted in increased bleeding and intracerebral hemorrhages and contributed to excess bleeding, including fatal bleeds, with initial clinical usage of the renally eliminated direct thrombin inhibitor dabigatran in frail elderly patients.11 Failure to recognize chronic kidney disease in the elderly patient with HF also is likely to be responsible for the high rate of hyperkalemia seen with use of spironolactone, especially at higher doses.12 Despite limitations of current methods to estimate renal clearance, routine estimation of creatinine clearance for dose adjustments of renally cleared medications and estimates of glomerular filtration for risk assessment before contrast administration, procedures, or surgery can guide efforts to reduce adverse effects and provides an opportunity for quality improvement. Consensus guidelines for oral dosing of renally excreted medications used frequently in the elderly population also may be helpful.13 Hepatic drug clearance is the net result of processes that include drug delivery to the liver (by portal vein and hepatic artery blood flow) and enzymatic transport into liver cells and enzymatic biotransformation and/or excretion via efflux transporter enzymes into the bile. These processes are influenced by heterogeneous factors that include genetic, disease, and environmental influences and metabolic enzymes that can be both inhibited and induced (see Chapter 9, Table 9-2), contributing to the lack of clinically validated algorithms to estimate hepatic and extrahepatic drug clearance or potential age-related changes. Drugs metabolized by the phase II conjugative reactions of glucuronidation (morphine, diazepam), sulfation (methyldopa), or acetylation (procainamide) do not appear to be affected by aging but show disease-related effects, may show frailty-related decreases, and show consistently lower clearance in women compared to men. In vitro, age-related changes are seen in phase I oxidative biotransformation by the membrane bound cytochrome P-450 (CYP) oxidative group of enzymes responsible for elimination of more than 50% of metabolized drugs. Cardiovascular drugs showing age-related decreases in CYP-mediated clearance in human investigations include alpha blockers (doxazosin, prazosin, terazosin), some beta blockers (metoprolol, propranolol, timolol), calcium channel blockers (dihydropyridines, diltiazem, verapamil), several hydroxymethyl glutaryl–coenzyme A (HMG-CoA) reductase inhibitors (fluvastatin, and in some studies, atorvastatin) and the benzodiazepine midazolam. Decreases in oxidative drug metabolism/clearance with age suggest that lower amounts of drug per unit time (or day) would be appropriate in older patients compared with younger patients, leading to the conventional recommendation to “start low and go slow” in the elderly. However, older age-related changes have not been detected in several population studies of patients including women and patients receiving multiple medications,14 suggesting that disease, environment, sex, and co-medications may have greater effects on CYP-mediated clearance than chronologic age. Data for humans on age-related changes in hepatic influx or efflux transporter enzymes are very limited. The lack of age-related changes in clearance of HMG-CoA reductase inhibitors (rosuvastatin, atorvastatin, fluvastatin) that are organic anion-transporting polypeptide (OATP) transporter substrates suggests age-related changes either are not marked or contribute less to overall substrate clearance than other factors. Therefore it is important to titrate to clinical effect after starting with reduced dosages in older patients. Attention has focused on genetic variation in explaining variability in drug metabolism, responses, and interactions (see Chapter 9). Warfarin and clopidogrel are examples of cardiovascular drugs metabolized by enzymes with relatively common pharmacogenetic variants. Polymorphisms of the CYP2C9 enzyme slow inactivation metabolism (clearance) of warfarin and polymorphic variants in the vitamin K–epoxide reductase complex (VKORC) can increase or decrease sensitivity to warfarin resulting in lower or higher dosing requirements (addressed later under Atrial Fibrillation: Anticoagulants) In general, the elimination half-life ( Age-related changes in protein binding of drugs are not usually found. Changes in free drug concentrations caused by competition of drugs for binding sites may occur but are transitory. Clinically significant examples involve warfarin, with changes in anticoagulation when additional drugs are added to warfarin therapy. Table 76-2 summarizes general guidelines for drug dosing in older patients. TABLE 76-2 Guidelines for Medication Prescribing in Older Patients Adverse drug events (ADEs) affect millions of people per year and account for up to 5% of hospital admissions. Adverse drug effects may manifest with “atypical” symptoms such as mental status changes and impaired cognition in the elderly. Literature reviews found ADE admission rates of 10.7% in elderly patients, with cardiovascular drugs accounting for approximately half, nonsteroidal anti-inflammatory drugs (NSAIDs) for 20%, and central nervous system drugs for 14%. A recent investigation of emergency hospitalizations for ADEs in older U.S. adults found that four medications were implicated, alone or in combination, in 67% of hospitalizations: warfarin (33.3%), insulins (13.9%), oral antiplatelet agents (13.3%), and oral hypoglycemic agents (10.7%).16 Medications previously recognized as “inappropriate” in the elderly17 were rarely implicated (1.2%). The risk for ADE-related emergency hospitalization increased with increasing age from 65 to older than 85 years of age. During non–ADE-related hospitalization, the odds ratio of severe ADEs with cardiovascular medications has been reported to be 2.4 times that of other medications. Both the risk of a medication error and that of a harmful or fatal outcome are highest in older adults.18 Other classes of drugs commonly associated with ADEs in community-dwelling elderly persons include diuretics, NSAIDs, selective serotonin reuptake inhibitors, beta blockers, and ACE inhibitors. In patients who are nursing home residents, drugs associated with ADEs are more frequently antibiotics, anticoagulants and antiplatelet drugs, atypical and typical antipsychotic drugs, antidepressants, antiseizure medications, or opioids. The most consistently identified risk factor for adverse drug interactions is the number of drugs prescribed, independent of age. Chronic administration of four drugs is associated with a risk of adverse effects of 50% to 60%; administration of eight or nine drugs increases the risk to almost 100% (Fig. 76-6). Although the goal is to prescribe as few drugs as possible in the elderly, the presence of multiple diseases and multi-drug regimens for common cardiovascular diseases often results in polypharmacy. The result is that approximately half of people older than 65 years of age have three or more medications prescribed on a daily basis, and 20% of patients 75 years and older have five drugs prescribed per outpatient encounter (www.cdc.gov). Even higher numbers of medications are prescribed for nursing home patients, averaging six to eight medications per day. Strategies that minimize the chance of drug interactions and adverse drug effects are thus essential. Pharmacokinetic interactions can lead to increased drug concentrations as a result of enzyme inhibition or to decreases secondary to enzyme induction. Interactions are more likely if co-administered medications are metabolized by or inhibit the same pathway (see Chapter 9 and also www.fda.gov/cder). The most potent inhibitors of the CYP oxidative enzymes are amiodarone (all isoforms) and droneradone (CYP3A), azole antifungal drugs itraconazole and ketoconazole (CYP3A), and protease inhibitors (CYP3A), followed by diltiazem (CYP3A) and erythromycin (CYP3A) (additional details are available online—e.g., at http://medicine.iupui.edu/clinpharm/ddis/main-table/). Coadministration of sulfonamide antibiotics with sulfonylureas can lead to hypoglycemia, in part because of CYP2C9 inhibition. Some drugs are administered as “prodrugs” and metabolized to active agents (many ACE inhibitors and clopidogrel). Inhibition of the antiplatelet effects of clopidogrel seen with coadministration of atorvastatin, decreasing clopidogrel activation by CYP3A, or proton pump inhibitors, which inhibit CYP2C19-mediated clopidogrel activation, has been reported. Induction of hepatic enzyme activity can lower concentrations of medications, leading to ineffective therapy. The antituberculosis drug rifampin is the most potent inducer of CYP1A and CYP3A. With mandatory screening for tuberculosis, treatment with rifampin may be initiated. Coadministered dosages of drugs cleared by CYP1A and CYP3A may need to be increased during rifampin administration and decreased upon discontinuation of rifampin. Markedly decreased cyclosporine levels and reduced clopidogrel inhibition of platelet aggregation during rifampin coadministration can occur. Other clinically relevant CYP inducers include carbamazepine (all CYPs), dexamethasone and phenytoin (CYP2C); caffeine, cigarette smoke, lansoprazole and omeprazole (CYP1A), St. John’s wort (CYP3A), and troglitazone (see http://medicine.iupui.edu/clinpharm/ddis/main-table/). Diet and drug and herb-drug interactions also occur. Because of the multiplicity of potential interactions and release of new medications and discovery of new interactions, use of pharmacy or computerized and online tools that provide comprehensive up-to-date information and guidelines for avoiding drug interactions is essential. Traditional text, online, and computer and smart phone applications are available from many sources—Lexicomp, the Medical Letter, the Physicians’ Desk Reference, Epocrates (available free of charge at www.epocrates.com), the FDA (the drug reactions section at www.fda.gov/cder), www.druginteractions.org, and http://medicine.iupui.edu/flockhart, among others. Many individual hospitals, health care systems, and pharmacies provide internal reference sources. Additional approaches that have been shown to reduce adverse drug reactions in older patients include involvement of pharmacy-trained personnel to assess the appropriateness of doses and medication counseling by members of a multidisciplinary care team. Algorithms have been developed for older patients to identify both medications that are potentially inappropriate and should be discontinued (STOPP criteria) and to identify ones that appear indicated and should be initiated (START criteria).19–21 Integrated medical record and pharmacy information, interactive databases, and computerized physician order entry with clinical decision support can reduce ADEs and improve medication therapy. By contrast, mandated drug utilization review efforts appear to be ineffective. Age-related changes in cardiovascular physiology and dynamics have a well-recogized impact on pharmacodynamics (see Table 76-1
Cardiovascular Disease in the Elderly
Demographics and Epidemiology
Pathophysiology
Medication Therapy: Modifications for the Older Patient
Loading Doses of Medications




Hepatic (and Intestinal) Clearance
 (Fig e76-1). Investigations of the use of genotyping to improve warfarin therapy to date have failed to identify frail elderly persons requiring the lowest warfarin dosing and cannot replace use of reduced initial doses and close monitoring in the very old.15 Clopidogrel is administered as a prodrug that requires activation metabolism by the polymorphic CYP2C19, and to a lesser extent CYP3A, for antiplatelet effects (see Chapter 82). Low activity pharmacogenetic variants result in less antiplatelet effect for any dose in carefully controlled investigations but the impact in the clinical setting is less striking leading to an uncertain role for pharmacogenetic screening to guide cardiovascular drug dosing at this time.
(Fig e76-1). Investigations of the use of genotyping to improve warfarin therapy to date have failed to identify frail elderly persons requiring the lowest warfarin dosing and cannot replace use of reduced initial doses and close monitoring in the very old.15 Clopidogrel is administered as a prodrug that requires activation metabolism by the polymorphic CYP2C19, and to a lesser extent CYP3A, for antiplatelet effects (see Chapter 82). Low activity pharmacogenetic variants result in less antiplatelet effect for any dose in carefully controlled investigations but the impact in the clinical setting is less striking leading to an uncertain role for pharmacogenetic screening to guide cardiovascular drug dosing at this time.
Elimination Half-Life
 ) for a drug increases with age, so the time between dosage adjustments needs to be increased in older patients before the full effect of a given dose can be assessed. Conversely, increased time is needed for complete drug elimination from the body and dissipation of drug effects.
) for a drug increases with age, so the time between dosage adjustments needs to be increased in older patients before the full effect of a given dose can be assessed. Conversely, increased time is needed for complete drug elimination from the body and dissipation of drug effects.

Adverse Drug Events and Drug Interactions
Pharmacokinetic Interactions
Adverse Pharmacodynamic Effects
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Cardiovascular Disease in the Elderly
76
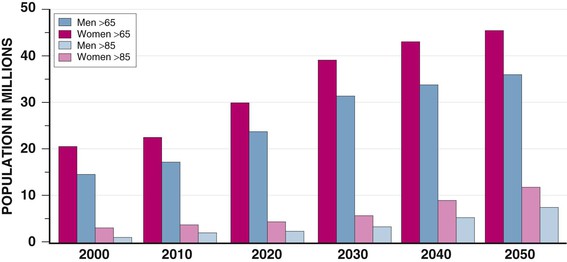
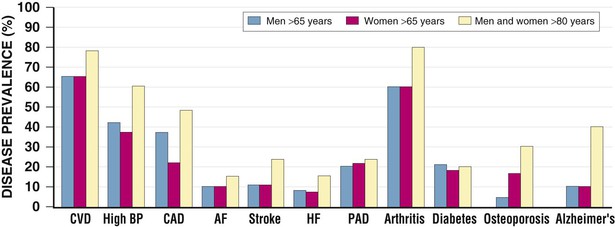
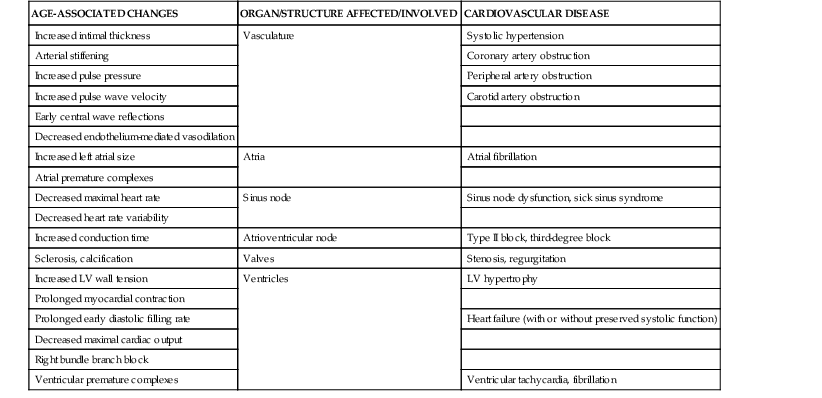
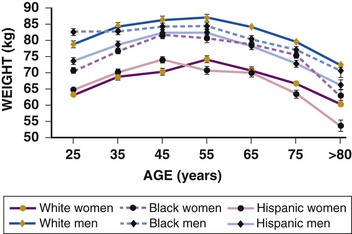
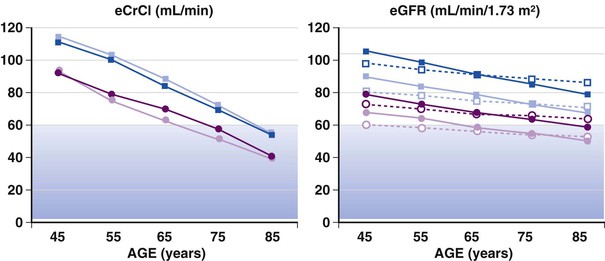
FIGURE 76-5 Estimates of creatinine clearance (eCrCl) using the C&G formula (left panel) and estimates of glomerular filtration rate (eGFR) using the MDRD simplified algorithm (represented by open symbols and dotted lines) and the CKD-EPI algorithm (represented by solid symbols and lines) for men and women 45 to 85 years of age (right panel). For calculations, mean weight and height by decade were obtained from U.S. survey data, serum creatinine was entered as 1.0 mg/dL (average for age older than 65 years from the survey data). Circles represent estimates for women; squares are estimates for men; lighter symbols are estimates for whites; and darker symbols represent estimates for African Americans. The shaded areas indicate GFR estimates of 30 to 59 mL/min/m2, classified as stage 3 renal disease or moderate GFR decrease. Cockcroft and Gault estimates show a steeper decline with age. Both formulas estimate lower clearance in women than in men and higher clearances in African Americans than in whites (based on average height and weights and the same creatinine). Data source: National Health and Nutrition Examination Survey (NHANES) (available at http://www.cdc.gov). (Modified from Schwartz JB: The current state of knowledge on age, sex, and their interactions on clinical pharmacology. Clin Pharmacol Ther 82:87, 2007.)
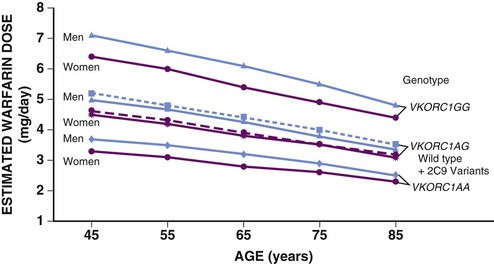
FIGURE e76-1 Warfarin dosing. Estimated warfarin dose by age, sex, and genotype. Estimates of doses are lower in women than in men of the same age and genotype, and age is predicted to affect dosage requirements for all genotypes. Variants of the VKORC can result in both increased sensitivity (1AA) and decreased sensitivity (1AG). Dotted lines represent data for both wild type CYP2C9 and its variants. Estimates were generated from an online calculator available at www.warfarindosing.org. (Modified from Schwartz JB: The current state of knowledge on age, sex, and their interactions on clinical pharmacology. Clin Pharmacol Ther 82:87, 2007.)
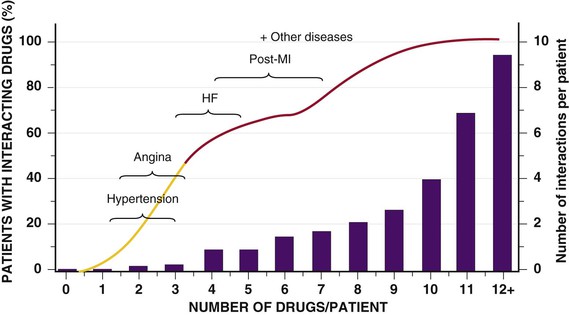
FIGURE 76-6 The relationship between the number of drugs consumed and drug interactions. Current guidelines for the pharmacologic management of patients with HF or recent MI place them at high risk for drug interactions. (From Schwartz JB: Clinical Pharmacology. Adult Clinical Cardiology Self-Assessment Program (ACCSAP) V, 2003. American College of Cardiology Foundation. Available at: http://www.cardiosource.org/. As modified from Nolan L, O’Malley K: The need for a more rational approach to drug prescribing for elderly people in nursing homes. Age Aging 18:52, 1989; and Denham MJ: Adverse drug reactions. Br Med Bull 46:53, 1990.)
