Alcohol consumption – potentially reversible cause
Infective – most commonly caused by Coxsackie A & B virus
Others – hypothyroidism, peripartum, chemotherapy, sarcoidosis
Clinical features
Heart failure is by far the most common presentation. Key feature is LV dilatation and systolic dysfunction
Investigations
ECG, Echo (gold standard), CXR
Management
Treat symptoms of heart failure (beta-blockers, ACE inhibitors, ARB, diuretics)
Anticoagulation if necessary
ICD and CRT in selected patients
Heart transplantation
14.2.1 Definition
Dilated cardiomyopathy is characterised by dilatation and systolic dysfunction of one or both ventricles where, in general, the LV is frequently affected in isolation. In addition to chamber dilatation, the ventricular wall is often abnormally thin.
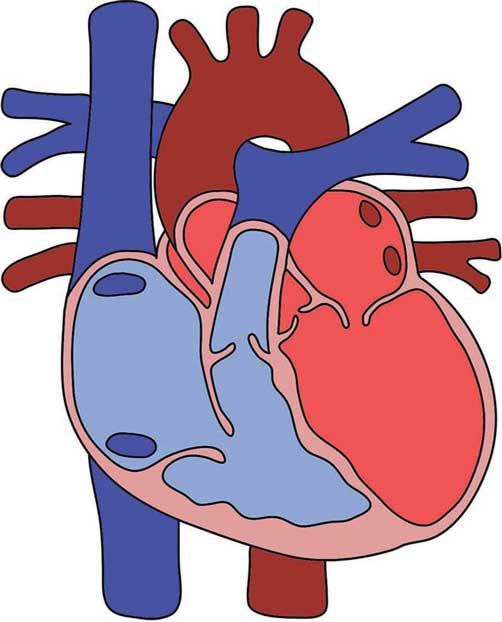
Figure 14.1 – Dilated cardiomyopathy.
14.2.2 Epidemiology
- 20–40 incidence per 100 000
- Male predominance 2:1
- Occurs with greater frequency in the Afro-Caribbean population
- Most commonly presents between 20 and 30 years of age.
// PRO-TIP //
Dilated cardiomyopathy is one of the most common reasons for requiring a heart transplant.
14.2.3 Aetiology
Key causes
- Idiopathic (50%): when primary and secondary causes have been eliminated
- Genetic: 25% inherited as autosomal dominant: a variety of single gene mutations have been identified. There are also autosomal recessive, X-linked (especially Duchenne’s and Becker’s muscular dystrophies), and mitochondrial inheritance patterns.
- Alcohol: Chronic alcohol consumption is implicated in the development of dilated cardiomyopathy in some individuals
- exact pathogenesis unknown, can present similar to other causes of dilated cardiomyopathy – always rule out alcohol as a factor because alcohol-related dilated cardiomyopathy is potentially reversible
- reducing alcohol consumption may show a dramatic improvement in ventricular function, but this varies between individuals.
- exact pathogenesis unknown, can present similar to other causes of dilated cardiomyopathy – always rule out alcohol as a factor because alcohol-related dilated cardiomyopathy is potentially reversible
// Why? //
Ethanol interferes with oxidative phosphorylation and fatty acid oxidation leading to cellular dysfunction.
- Infective: frequently occurs as a sequela of viral myocarditis
- viral causes include: parvovirus, Coxsackie A and B, influenza, adenovirus, echovirus, cytomegalovirus and HIV
Non-viral causes include: Chagas disease (Trypanosoma cruzi ): endemic to South America, which causes megaoesophagus, megacolon and dilated cardiomyopathy, and Lyme disease.
// PRO-TIP //
Dilated cardiomyopathy in Chagas disease develops 10–20 years after being infected with the parasite.
Other causes
- The number of causes of dilated cardiomyopathy is virtually limitless. The important ones are:
- hypothyroidism
- peripartum cardiomyopathy
- chemotherapy (doxorubicin/Adriamycin, 5-fluorouracil and trastuzumab/Herceptin)
- sarcoidosis.
- hypothyroidism
14.2.4 Pathophysiology
The pathogenesis of dilated cardiomyopathy is unclear.
Enlargement of all four chambers may occur, with the LV most commonly affected.
Dilatation is associated with decreased contractile function.
EXAM | As dilation occurs, and the heart becomes functionally impaired, the body attempts to compensate with:
|
14.2.5 Clinical features
Key features
- Asymptomatic: may be an incidental finding
- Presents with heart failure symptoms: breathlessness, peripheral oedema, fatigue, syncope, sporadic chest pain
- Arrhythmia: e.g. atrial fibrillation (AF) or sudden cardiac death due to ventricular arrhythmia
- Thromboembolism.
EXAM | Remember to ask about a history of viral illness or myocarditis in the past and a positive family history may be helpful. |
Examination findings:
- Presents with a displaced heart beat secondary to LV dilatation
- Signs of heart failure (refer to Chapter 10)
- S3 and S4 gallop.
14.2.6 Investigations
First-line
Initial investigations are as for heart failure:
- ECG: changes are non-specific
- CXR: features of heart failure, cardiomegaly
- Bloods: including LFTs, electrolytes, TFTs, and ferritin (note that haemochromatosis is an important reversible cause)
- Echocardiography: gold standard.
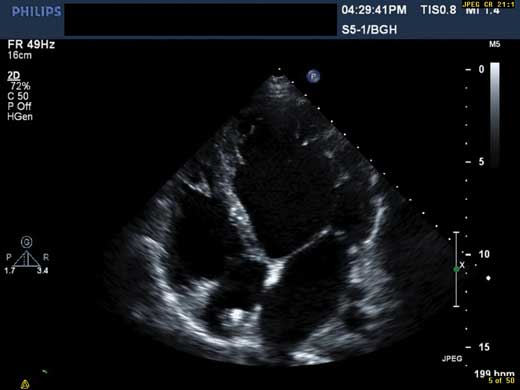
Figure 14.2 – Left ventricular dilatation seen on echocardiography.
// PRO-TIP //
The key lies in unexplained left ventricular dilatation. This may be difficult to distinguish from ischaemic cardiomyopathy. It is an important differentiation that can be made using angiography and/or MRI.
Second-line
- Cardiac biopsy can establish definitive diagnosis but its use is controversial
- Cardiac MRI may be useful.
14.2.7 Management
The treatment of dilated cardiomyopathy aims to:
- Treat identifiable underlying cause
- Manage heart failure symptoms
- beta-blockers and ACE inhibitors/ARBs improve survival
- ACEi/ARBs also reduce the risk of sudden arrhythmic death
- loop and thiazide diuretics
- spironolactone also improves survival
- beta-blockers and ACE inhibitors/ARBs improve survival
- Prevent complications
- anticoagulation is not routinely offered. Generally prescribed if patients have AF or evidence of an LV thrombus, for example.
- anti-arrhythmics
- implantable cardioverter defibrillator (ICD) and cardiac resynchronisation therapy (CRT): refer to Chapter 10 for the section on CRT and to Chapter 11 for the section on ICDs
- heart transplantation may eventually be an option for the select few where maximal medical therapy has failed.
- anticoagulation is not routinely offered. Generally prescribed if patients have AF or evidence of an LV thrombus, for example.
// Why? //
Stasis of blood flow in the ventricles may predispose to thromboembolism.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


