Later that evening she develops recurrent nonsustained polymorphic ventricular tachycardia. Which of the following intravenous medications may be useful in treating this patient’s dysrhythmia?
A. Procainamide
B. Magnesium sulfate
C. Sotalol
D. Quinidine
E. Dofetilide
2. An 8-year-old boy is diagnosed with long QT syndrome (LQTS) associated with a mutation in sodium channel gene SCN5A following an evaluation for unexplained syncope. His baseline QTc interval is 490 ms. He undergoes placement of an ICD/pacemaker. While in the ICU, he has frequent episodes of nonsustained polymorphic ventricular tachycardia, which are suppressed by intravenous lidocaine administration. Which of the following oral medications would be the best outpatient treatment for this patient?
A. Quinidine
B. Sotalol
C. Dofetilide
D. Procainamide
E. Mexiletine
3. An 18-year-old male with a bileaflet aortic valve mechanical prosthesis that was placed 2 years ago is scheduled for an elective urological operation. He has no previous history of clots, arrhythmia, stroke, or transient ischemic attacks. On a recent echocardiogram, his left ventricular ejection fraction was 55%. Which of the following statements is most consistent with the 2008 recommendations from the American College of Cardiology for perioperative anticoagulation in this setting?
A. Warfarin should be stopped 48 hours prior to procedure, and he should be bridged with unfractionated heparin
B. Warfarin should be stopped 48 hours prior to procedure, and he should be bridged with subcutaneous heparin
C. Warfarin should be stopped 48 hours prior to procedure, and he should be started on Plavix
D. Warfarin should be stopped 72 hours prior to procedure, and no heparin bridging is necessary
E. Warfarin should be stopped 72 hours prior to procedure, and he should be bridged with unfractionated heparin. Heparin should be stopped 4 to 6 hours prior to surgery.
4. A 16-year-old male with a previously repaired partial AV canal defect and cleft mitral valve undergoes mechanical bileaflet mitral valve prosthesis placement for symptomatic severe mitral valve regurgitation. His discharge echocardiogram shows a left ventricular ejection fraction of 60%. Based on the 2008 American College of Cardiology recommendations for postoperative anticoagulation, which of the following is the best long term anticoagulation strategy for this patient?
A. Warfarin (aim for INR between 2 and 3) alone; no aspirin
B. Warfarin (aim for INR between 2.5 and 3.5) alone; no aspirin
C. Warfarin (aim for INR between 2 and 3) along with aspirin 325 mg
D. Warfarin (aim for INR between 2.5 and 3.5) along with aspirin 81 mg
E. Warfarin (aim for INR between 2 and 3) along with aspirin 325 mg
5. An 18-year-old female with a history of parachute mitral valve and mechanical mitral prosthesis placement takes warfarin 4 mg/day. She has just learned that she is 14 weeks pregnant and wishes to continue with her pregnancy. Which of the following treatment options would you advise?
A. Strongly recommend elective termination of the pregnancy
B. Discontinue warfarin for the remainder of the pregnancy, then restart in the postpartum period
C. Continue warfarin for the remainder of the pregnancy
D. Discontinue warfarin now and restart at 25 to 30 weeks gestation, treating with subcutaneous heparin in the interim
E. Continue warfarin till 36 weeks gestation, then treat with continuous intravenous Heparin and deliver in 2 to 3 weeks
6. A 9-year-old patient with myocarditis, cardiomegaly, and reduced left ventricular systolic function develops a dry cough without other respiratory symptoms after starting an angiotensin-converting enzyme (ACE) inhibitor for treatment of heart failure. Which of the following is the most likely mechanism of cough due to the medication?
A. Increased bradykinin
B. Inhibition of Na+-K+ ATPase pump
C. Inhibition of calcium entry into vascular smooth muscle cells
D. Inhibition of activation of angiotensin II receptors
E. Increased production of angiotensin II
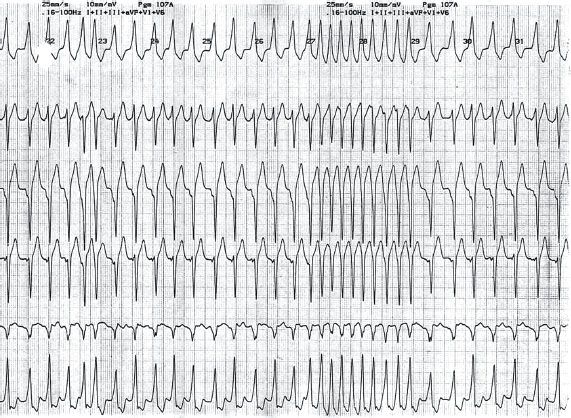
7. A 7-year-old well child with a recent history of palpitations is admitted to the ED with shortness of breath and tachyarrhythmia. He has no previous history of syncope or exercise induced symptoms. His ECG shows an irregularly irregular wide complex tachycardia with variable ventricular rates (150 to 300 bpm), as seen in Figure 10.2. No
P waves are discernible on the ECG. Vagal maneuvers have failed. His blood pressure (BP) is 100/60 mm Hg. The patient has been cardioverted three times, with transient return to sinus rhythm, but the tachycardia recurs. Which of the following medications would be most likely to treat this patient’s arrhythmia?
A. IV adenosine
B. IV digitalis
C. IV amiodarone
D. IV β-blocker
E. IV diltiazem
8. A 10-month-old female presents 1-week after hospital discharge following repair of tetralogy of Fallot (TOF). Her parents describe a 3-day history of vomiting without diarrhea. She has not had a fever. Cardiac monitoring reveals the rhythm shown in Figure 10.3.
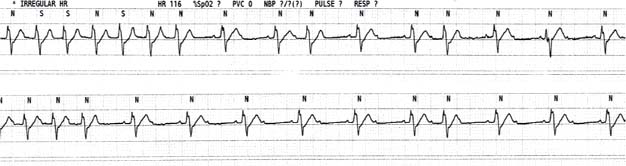
Which of the following medications is most likely to cause this patient’s symptoms and electrocardiographic findings?
A. Digoxin
B. Propranolol
C. Furosemide
D. Amiodarone
E. Chlorothiazide
9. A 13-year-old boy with a history of catecholaminergic polymorphic ventricular tachycardia (CPVT) is admitted to the ICU after an episode of syncope with exertion. In the ICU, he is noted to have frequent episodes of polymorphic ventricular tachycardia associated with hypotension. Which of the following is the best antiarrhythmic therapy for this child?
A. Amiodarone
B. Lidocaine
C. β-Blocker
D. Calcium channel blocker (CCB)
E. Digoxin
10. A 13-month-old male referred to you for a heart murmur is diagnosed with a secundum atrial septal defect (ASD) measuring 6 mm. He was born at 38 weeks of gestation and has been thriving well without any symptoms. There is mild right heart enlargement on echocardiogram, and right ventricular systolic pressure is estimated to be 30 mm Hg. His mom, who is a pediatric nurse, is concerned about RSV and wants to know whether her son needs any palivizumab prophylaxis for the RSV season. Which of the following is the most appropriate answer?
A. Because he is over 1 year old, he does not need RSV prophylaxis
B. RSV prophylaxis would only be recommended if he had a prior history of RSV infection
C. RSV prophylaxis is not recommended for his specific situation
D. RSV prophylaxis is recommended for him until he is 2 years old
E. RSV prophylaxis would be recommended for him if he were exposed to cigarette smoke at home
11. You are evaluating a 14-month-old female in the outpatient pediatric cardiology clinic. She was diagnosed with hypoplastic left heart syndrome after a full-term delivery. She underwent a stage I Norwood procedure and a stage II superior cavopulmonary anastomosis (Glenn procedure) at 6 months of age. She is currently doing well. Her only medication is aspirin. Her resting oxygen saturation is 80%. Echocardiogram shows normal right ventricular size and function and a patent Glenn shunt with appropriate flow in the pulmonary arteries. She received palivizumab prophylaxis last RSV season. Her mother wants to know whether palivizumab would be helpful during the current RSV season. Which of the following is the most appropriate response to her question?
A. Palivizumab prophylaxis has been shown to reduce the risk of RSV infection and is therefore beneficial
B. Palivizumab prophylaxis has been shown to reduce mortality rate from RSV in patients with congenital heart disease and therefore is recommended
C. Palivizumab would protect her from most viral infections including influenza A and B
D. Palivizumab would likely decrease her need for hospitalization if she contracted RSV and therefore is recommended
E. Palivizumab is not recommended after 1 year of age
12. A 5-month-old female with dilated cardiomyopathy is started on furosemide. This medication acts by inhibiting which of the following ion channels?
A. Na+-2Cl−-K+ cotransporter in the loop of Henle
B. Na+-Cl− cotransporter in the proximal tubule
C. Na+-K+ ATPase pump in the distal tubule
D. Na+-H+ cotransporter in the loop of Henle
E. Na+-Ca2+ cotransporter in the proximal tubule
13. A 17-year-old previously healthy female presents to the ED with a 2-day history of chest pain. Her electrocardiogram shows diffuse ST segment elevation and PR segment depression suggestive of pericarditis. Echocardiogram shows normal biventricular size and function with a small pericardial effusion. There is no history of recent fever, rash, sore throat, or joint pains. Which of the following is the best treatment option for this patient?
A. Aspirin 325 mg 4 times/day for 4 weeks followed by gradual taper over the next 2 weeks
B. Prednisone 1 mg/kg/day followed by tapering after 2 weeks once patient is asymptomatic
C. Colchicine therapy for 4 to 6 days
D. Ibuprofen 600 to 800 mg 3 times a day
E. Plavix 75 mg daily for 2 weeks
14. A 5-day-old neonate with hypoplastic left heart syndrome is being cared for in the cardiac ICU on the second postoperative day following a Norwood operation with right modified Blalock–Taussig shunt. Arterial blood gas (on FiO2= 21%) shows a pH of 7.2. PO2 is 42 mm Hg, PCO2 is 45 mm Hg, SpO2 is 80%, and hemoglobin 14 g/dL. Near infrared spectroscopy (NIRS) probes consistently show saturations in the 40% range. ECG shows sinus tachycardia with a heart rate (HR) in the 180 s. Arterial BP is 78/58 mm Hg. Chest x-ray shows no evidence of pulmonary congestion or significant infiltrates and lung fields are well expanded. The patient is on milrinone 0.4 mcg/kg/min and norepinephrine 1 mcg/kg/min. Urine output over the past 6 hours has averaged 1 cc/kg/hour. Limited bedside echo shows no significant pericardial effusion. The patient just received two 10 ml/kg boluses of normal saline. Which of the following interventions is most likely to benefit this patient?
A. IV furosemide
B. Decrease in norepinephrine infusion rate
C. IV β-blocker therapy
D. Decrease in milrinone infusion rate
E. Increasing the inspired FiO2 concentration
15. A 10-month-old infant is treated for Kawasaki disease (KD) with intravenous immunoglobulin (IVIG) and aspirin. Which of the following statements regarding use of steroids in KD is most accurate?
A. A 24-hour continuous IV steroid infusion may be considered in addition to IVIG as primary therapy
B. Oral steroids may be used instead of aspirin if the patient remains afebrile but shows persistent elevation of acute inflammatory markers (ESR, CRP)
C. Steroids are contraindicated in Kawasaki patients
D. IV steroids may be considered for primary therapy in this infant patient
E. IV steroids may be considered if the patient has persistent or recrudescent fever after two doses of IVIG
16. A 7-year-old girl whose parents recently emigrated from Mexico is diagnosed with acute rheumatic fever (RF). She complains of mild chest pain, but no shortness of breath. Cardiac examination reveals normal S1 and S2, with a soft holosystolic murmur at the apex. Neck veins do not appear to be distended. Abdominal exam shows no organomegaly. Echocardiogram shows small pericardial effusion, mild-to-moderate mitral valve regurgitation, mild aortic valve regurgitation, mildly dilated left ventricle with an ejection fraction of 60%. Which of following treatment regimens should be initiated in the above patient?
A. IV steroids
B. Oral steroids
C. High-dose aspirin
D. β-Blocker therapy
E. IVIG + aspirin
17. Which of the following statements is true regarding immunosuppressive medications used in patients following heart transplantation?
A. Sirolimus is a calcineurin inhibitor
B. Tacrolimus is not available for intravenous use
C. Sirolimus acts by blocking gene transcription
D. Tacrolimus has been associated with improved survival over cyclosporine
E. Sirolimus offers no advantage in terms of nephrotoxicity over cyclosporine
18. A 7-year-old girl who was appropriately treated for her first episode of RF with mild carditis is followed up at 3 months, 6 months, and then at 1 year. Serial follow-up echocardiograms show no residual pericardial effusion, trivial mitral valve regurgitation, no aortic valve regurgitation, normal left ventricular chamber size, and function. She is maintained on RF antibiotic prophylaxis and continues to remain asymptomatic without any recurrence of streptococcal sore throat. If there is no echocardiographic evidence of worsening ventricular or valvular function, which of the following is the best recommendation for ongoing antibiotic prophylaxis?
A. Antibiotic prophylaxis should be continued for 5 years
B. Antibiotic prophylaxis should be continued for 10 years
C. Antibiotic prophylaxis should be continued until she is 21 years of age
D. Antibiotic prophylaxis should be continued until she is 40 years of age
E. She will need lifelong antibiotic prophylaxis
19. According to the latest AHA/ACC guidelines, infective endocarditis (IE) prophylaxis is recommended in which of the following clinical scenarios?
A. 7-year-old patient who has undergone cardiac transplantation 18 months ago with trivial tricuspid valve regurgitation prior to dental extraction
B. 8-year-old patient who has undergone device closure of ASD 4 months ago with residual shunt at the site of prosthetic device who is scheduled to undergo an upper gastrointestinal endoscopy
C. 9-year-old patient with TOF who underwent complete repair at 6 months of age and has an RV to PA conduit and is scheduled to have dental brace placement
D. 8-year-old patient with prosthetic mitral valve with previous history of IE who is scheduled for an outpatient cystoscopy
E. 12-year-old patient who has undergone percutaneous PDA closure 4 months ago who needs a root canal
20. A 14-year-old male is referred to your clinic for management of elevated LDL cholesterol. 12 months ago his LDL level was 196 mg/dL, and he was advised appropriate dietary intervention and weight reduction regimen. At present his LDL level is 202 mg/dL, HDL is 28 mg/dL, and triglycerides are 150 mg/dL. His BMI is 31 kg/m2 and his TSH level is normal. He has been compliant with his diet and exercise program and has lost 3 kg over the past year. He was adopted and therefore family history is not well known. Which of the following statements is most accurate?
A. Continued dietary intervention alone will likely significantly reduce his LDL level over the next 6 months
B. Oral statin therapy should be strongly considered
C. Oral niacin therapy is the best first-line option due to its side effect profile
D. Fibric acid derivatives should be considered
E. If drug therapy is considered, bile acid binding resins would be first-line therapy given their favorable safety and side effect profile
21. A 16-year-old male recently diagnosed with hypertrophic cardiomyopathy (HCM) presents for evaluation. No other associated medical conditions are present. Medications include multivitamins. He is asymptomatic at rest, but complains of shortness of breath with exertion. There is no history of syncope/pre-syncope or family history of HCM or sudden death. His resting HR is 80 bpm and BP is 130/80 mm Hg. His echocardiogram shows a septal thickness of 26 mm, ejection fraction = 70%, left ventricular outflow tract maximum instantaneous gradient is 60 mm Hg. Cardiac MRI shows minimal late gadolinium enhancement. Recent Holter report showed frequent single PVCs, but no sustained tachycardia. On the basis of the above information, which of the following is the best initial treatment for this patient?
A. Septal myectomy + ICD ± medication
B. Septal myectomy ± medication
C. Oral Furosemide therapy
D. β-Blocker therapy
E. Treatment with Nifedipine
22. Which of the following medications used in heart transplant recipients can inhibit smooth muscle proliferation and may have the advantage of inhibiting coronary allograft vasculopathy?
A. Pulse methylprednisolone
B. Sirolimus
C. Antithymocyte globulin (ATG)
D. Cyclosporine
E. Tacrolimus
23. A 3-day-old term neonate with hypoplastic left heart syndrome is initiated on cardiopulmonary bypass for Norwood palliation. Which of the following medications would be most likely to increase systemic perfusion in this patient?
A. Milrinone
B. Epinephrine
C. Clonidine
D. Dopamine
E. Norepinephrine
24. An 8-year-old male with a history of heart transplant performed 3 years ago is admitted in the ER for management of respiratory distress. Vitals: HR is 120 bpm, respiratory rate is 40/min with intercostal and subcostal recessions, BP is 75/40 mm Hg, SpO2 is 85% on oxygen, capillary refill time is >3 s and peripheries feel cold. Chest x-ray shows bilateral hazy lung fields. Patient’s home medications include tacrolimus, low-dose oral prednisone, carvedilol, and enalapril. The treating team is planning to intubate and mechanically ventilate him. Which of the following statements regarding treatment options is accurate in this situation?
A. A combination of intravenous morphine and succinylcholine is the best choice for sedation and muscle relaxation
B. A combination of intravenous fentanyl and pancuronium is the best choice for sedation and muscle relaxation
C. Ketamine is contraindicated in this setting
D. Thiopental may be a useful drug in this scenario
E. Pancuronium is a depolarizing neuromuscular blocker and should not be considered because of its unfavorable profile on HR and BP
25. An 15-year-old male presents to the ER with fast HRs and some shortness of breath. His ECG shows regular narrow complex tachycardia (HR 235 bpm) without discernible p waves. He was discharged 24 hours ago from the hospital following management of asthma exacerbation and received treatment in the intensive care unit. Vagal maneuvers have failed to bring down his HR. Which of the following statements regarding adenosine is true?
A. Adenosine should be slowly pushed to avoid bronchospasm
B. If bronchospasm results, it will only last several seconds, then resolve
C. If the patient had received a heart transplant, double the typical dose of adenosine should be used
D. Transient hypertension may result from adenosine administration
E. Flushing of the face is a common side effect
26. A 13-year-old female is newly diagnosed with idiopathic pulmonary arterial hypertension. She experiences shortness of breath at rest and has severe right ventricular enlargement with severe dysfunction. She is started on IV epoprostenol, oral sildenafil, and ambrisentan. Which of the following is the correct statement among the following regarding her pharmacological treatment?
A. Ambrisentan is an endothelin A receptor agonist
B. Epoprostenol is a prostaglandin (PGE2) analogue
C. Ambrisentan does not affect cytochrome P450 enzyme activity
D. Sildenafil is phosphodiesterase 3 inhibitor
E. Multi-drug combination therapy has been shown to improve survival in children with idiopathic pulmonary hypertension
27. A 16-year-old male is evaluated by his cardiologist following a recent episode of unexplained syncope. His resting ECG and echocardiogram are normal, and the history is not typical for vasovagal syncope. His father is an immigrant from South-East Asia and was diagnosed with Brugada syndrome 1 year ago. Which of the following tests would be helpful in making a definitive diagnosis in this patient?
A. Epinephrine challenge test
B. Cardiac MRI
C. Isoproterenol provocative test
D. Provocative testing with procainamide
E. Exercise test
28. A 10-year-old female with known LQTS type 1 (LQTS 1) presents with status epilepticus to the emergency department. She is on oral nadolol therapy. Her ECG shows sinus rhythm (120 bpm) and her resting QT interval is 500 ms. The ER doctor prepares to administer IV phenytoin and consults the cardiologist regarding the safety of phenytoin use in the patient. Which of the following statements is accurate with regards to the current patient scenario?
A. Phenytoin can prolong the QT interval and is therefore not safe in the patient
B. Patient should be started on IV amiodarone before starting phenytoin
C. Intravenous β-blocker can be administered concurrently with phenytoin drip
D. Phenytoin has cardiac effects similar to mexiletine
E. Phenytoin blocks cardiac potassium channels
29. An 18-year-old female patient with a history of repaired Ebstein’s anomaly is admitted to the ER with shortness of breath and a tachycardia (HR of 150 bpm). She is found to be in atrial flutter with variable conduction on ECG evaluation. She is hemodynamically stable. An echocardiogram done 1 year ago showed normal left ventricular function with mild right ventricular dysfunction. Which of the following options is most appropriate in the immediate management of the patient?
A. Flecainide
B. Diltiazem
C. Disopyramide
D. Heparin, transesophageal echocardiogram and preparation for urgent electrical cardioversion
E. Labetalol
30. Which of the following drugs is a calcium-sensitizing agent?
A. Verapamil
B. Digoxin
C. Levosimendan
D. Milrinone
E. Nesiritide
31. A newborn baby is noted to be bradycardic with a HR of 40 bpm. An ECG shows complete AV block. Which of the following medications would be most useful to increase the HR in this scenario?
A. Milrinone infusion
B. Atropine infusion
C. Digoxin infusion
D. Isoproterenol infusion
E. Dobutamine infusion
32. A 15-year-old female with known Marfan syndrome is admitted to the intensive care unit with acute severe mitral valve regurgitation in the setting of a flail mitral valve leaflet. She is felt to be in a low cardiac output state with pulmonary edema. Her EF is 70%. Which of the following medications would be most helpful in improving her cardiac output acutely prior to surgery?
A. Nitroprusside infusion
B. Intravenous Lasix
C. Vasopressin infusion
D. Intravenous digoxin
E. Dopamine infusion
33. A 3-month-old child with unrepaired TOF is referred to the ER by his pediatrician because his oxygen saturation during a well-child visit was only 62%. On examination, the patient is cyanotic but alert. His parents note that he has been less active for the past few days. His HR is 180 bpm, SpO2 is 55% to 60%, respiratory rate is 40/min, and BP is 88/50 mm Hg. The lungs are clear on auscultation and a grade 3/6 harsh systolic ejection murmur is heard over the precordium. He is not on any medications. His lab work done at his pediatrician’s office is available: Na 142, K 3.8, chloride 105, bicarbonate 26, BUN 15, creatinine 0.6, hematocrit 26, WBC 9000, platelet count is 350, 000. Which of the following therapies can be expected to improve the patient’s condition?
A. Intravenous propranolol
B. Phenylephrine infusion
C. Packed red blood cell transfusion
D. Morphine administration
E. Intravenous furosemide
34. A 2-day-old child with hypoplastic left heart syndrome is started on prostaglandin E1 (PGE1). The parents have opted for a cardiac transplantation for the child and the cardiology team has decided to maintain him on PGE1 until a donor heart becomes available for transplantation. Which of the following statements is true with regard to the side effects of PGE1?
A. Assisted ventilation may be necessary because of primary hypoxia
B. Hypothermia is a potential side effect
C. Patient needs to be monitored for hypertension
D. Seizures are not associated with administration of PGE1
E. Cutaneous vasodilation and edema can develop as a side effect
35. Which of the following drugs used in the treatment of Marfan’s syndrome blocks TGF-β signaling?
A. Losartan
B. Propranolol
C. Enalapril
D. Verapamil
E. Spironolactone
36. An 18-year-old male with dilated cardiomyopathy and LVEF of 30% comes for a follow-up outpatient evaluation. He has a chronically elevated potassium. Which of the following medications would be indicated considering his hyperkalemia?
A. Eplerenone
B. Spironolactone
C. Captopril
D. Metoprolol
E. Enalapril
37. A 16-year-old patient who received a cardiac transplantation 10 years ago is managed as an outpatient. His LVEF has been in the 25% range for the past 1 year, and he is thought to have advanced coronary allograft vasculopathy. A 24-hour ECG monitoring shows repeated episodes of atrial flutter. He is currently on the following oral medications: carvedilol, atenolol, spironolactone, digoxin, enalapril, warfarin, cyclosporine, oral steroids. The treating cardiologist elects to start him on amiodarone. Which of the following statements is correct with respect to drug interactions in the setting of amiodarone therapy?
A. Digoxin dose does not need to be adjusted when adding amiodarone
B. Enhanced AV nodal conduction can occur and can result in rapid ventricular response in the setting of atrial arrhythmias
C. Cyclosporine levels may be elevated after beginning amiodarone
D. INR should be checked periodically as it may become subtherapeutic
E. Steroid dose should be decreased after adding amiodarone
38. Which of the following statements is true regarding the antiarrhythmic action of amiodarone?
A. It shortens the QTc interval
B. It produces some degree of calcium channel blockade
C. It activates cardiac sodium channel
D. It has vagolytic effects
E. Presence of hypokalemia reduces its pro-arrhythmic potential
39. A 11-year-old female who received a heart transplant 10 years ago is maintained on tacrolimus, prednisone, and sirolimus. Which of the following statements is true with regard to associated side effects?
A. The use of sirolimus is not associated with bone marrow suppression
B. Lipid abnormalities typically do not develop until adolescence
C. Tacrolimus is more associated with the development of diabetes mellitus than cyclosporine
D. Thiazides are the first line anti hypertensive agents in heart transplant recipients
E. Sirolimus is more nephrotoxic than cyclosporine and tacrolimus
40. Which of the following drugs lowers pulmonary vascular resistance (PVR)?
A. Nitrous oxide
B. Ketamine
C. Prostacyclin
D. Dopamine
E. Norepinephrine
41. A 4-year-old female who underwent a Fontan procedure 6 days ago develops acute arterial thrombosis of her right big toe. An emergency echocardiogram shows normal systemic ventricular function without any thrombus and a patent Fontan pathway. She is receiving heparin 10 units/kg/h through a central catheter in her internal jugular vein. She is currently on aspirin 81 mg/day, milrinone, furosemide. She has been receiving frequent doses of fentanyl for her severe pain. Her CBC today shows a hemoglobin of 12.8, white blood cell count of 12, 000, and a platelet count of 60, 000. Two days prior, her platelet count was 300, 000. There is no evidence of any bleeding. The intensivist orders additional tests to clarify the diagnosis. Which of the following is most likely responsible for her drop in platelets?
A. Milrinone
B. Furosemide
C. Aspirin
D. Heparin
E. Fentanyl
42. Which of the following medications is correctly listed with its teratogenic effect?
A. Lithium: left-sided obstructive lesions
B. Amiodarone: permanent fetal complete heart block
C. Warfarin: defects in central nervous system
D. ACE inhibitors: right-sided obstructive lesions
E. High dose folic acid: neural tube defects
43. An 18-year-old male patient with a history of TOF that was repaired 13 years ago presents to the emergency room with vomiting and complaints of visual disturbances (flashing lights and halos) and feeling dizzy. He has a history of underlying mild renal dysfunction. He was recently diagnosed with infectious mononucleosis. His oral intake has been reduced for the past few days, but he has been taking his digoxin, furosemide, and aspirin regularly. His HR is 40 bpm, respiratory rate is 18/min, SpO2 is 98%, and BP is 85/40 mm Hg. Electrocardiogram shows underlying sinus rhythm, right bundle branch block with no evidence of peaked T waves, 3:1 AV block, ventricular bigeminy, and frequent 3 to 4 beat runs of premature ventricular contractions. Which of the following is the most likely to reveal the source of his symptoms?
A. Serum potassium level
B. Liver function tests
C. Beta natriuretic peptide (BNP) level
D. Aspirin level
E. Digoxin level
44. A 6-year-old female is 2 days post repair of coarctation of aorta and subaortic membrane resection. She is intubated and appears comfortable on the ventilator (FiO2 40%). She is noted to have persistently elevated BP (190–200/100–110 mm Hg) despite use of intravenous fentanyl and furosemide. Her HR is 100 bpm and SpO2 is 90%. Chest x-ray shows some atelectasis in both lung fields. Her morning labs are as follows: hemoglobin 8.5, WBC 9000, platelets 150, 000, BUN 38, creatinine 1.9, ALT 250, AST 300. Her outpatient medications include the following: methylphenidate, albuterol prn, fluticasone/salmeterol twice daily, and montelukast daily. Which of the following treatment options would be best for this patient?
A. Inhaled nitric oxide therapy
B. Intravenous nicardipine
C. Intravenous labetalol
D. Sodium nitroprusside infusion
E. Dexmedetomidine infusion
45. A 6-year-old male undergoes percutaneous pulmonary valvotomy for valvular pulmonary stenosis. His baseline SpO2 is 98% on room air. His pre-procedure echocardiogram had demonstrated a mean gradient of 55 mm Hg across the valve, right ventricular hypertrophy with normal systolic function, patent foramen ovale, normal branch pulmonary arteries, and normal left ventricular chamber size/systolic function. Following his procedure in the catheterization laboratory, his peak to peak gradient decreased from 80 mm Hg to 30 mm Hg and SpO2 was 95% (room air). Three hours later he is noted to be desaturating with SpO2 in the 80s on room air and is not with poor peripheral perfusion. Which of the following treatment options would be most helpful in this patient?
A. Inhaled nitric oxide therapy
B. Milrinone therapy
C. Phenylephrine therapy
D. Intravenous β-blocker
E. Intravenous furosemide
46. A 14-year-old patient on a statin to lower his cholesterol presents with fatigue, back pain, and soreness in the arms and legs. Which of the following lab values is most likely to reveal the etiology?
A. Serum potassium level
B. Creatine kinase level
C. Serum creatinine
D. Serum cholesterol level
E. Complete blood count
47. Which of the following is the location of action of chlorothiazide?
A. Distal tubule
B. Proximal tubule
C. Loop of Henle
D. Afferent renal artery
E. Efferent renal artery
48. Which of the following would most likely be helped by intravenous furosemide?
A. Hypokalemia
B. Hypomagnesemia
C. Hypercalcemia
D. Hypernatremia
E. Metabolic acidosis
49. What is the mechanism of action of acetazolamide?
A. Inhibits sodium reabsorption in the loop of Henle
B. Carbonic anhydrase inhibitor
C. Arginine vasopressor agonist
D. Inhibits chloride reabsorption at the distal tubule
E. Direct increase in renal artery blood flow
50. Which of the following does NOT have its primary mechanism of action at the loop of Henle?
A. Ethacrynic acid
B. Furosemide
C. Bumetanide
D. Torsemide
E. Metolazone
ANSWERS
1 ANSWER: B. Prolonged QT interval is noted on the given ECG. The patient probably has LQTS in the given clinical scenario.
Class IIa recommendation: Management with intravenous magnesium sulfate is reasonable for patients who present with LQTS and few episodes of torsades de pointes. Magnesium is unlikely to be effective in patients with a normal QT interval (level of evidence: B). The other agents in the given scenario tend to prolong QT interval and therefore are not recommended.
2 ANSWER: E. The patient in this scenario likely has type-3 LQTS.
Class IIb recommendation: Intravenous lidocaine or oral mexiletine may be considered in patients who present LQT3 and torsades de pointes (level of evidence: C). The other agents in the given scenario tend to prolong QT interval and therefore are not recommended.
3 ANSWER: D. In the given scenario, the patient has a bileaflet mechanical aortic valve without any additional risk factors for thromboembolism (see below). The recommendation as per the ACC/AHA 2008 guideline is to stop warfarin 72 hours prior to the procedure without any need for heparin bridging. Class I recommendations for perioperative anticoagulation strategy as per ACC/AHA 2008 guidelines is quoted below.
Class I recommendation:
1. In patients at low risk of thrombosis, defined as those with a bileaflet mechanical AVR with no risk factors, * it is recommended that warfarin be stopped 48 to 72 h before the procedure (so the INR falls to less than 1.5) and restarted within 24 h after the procedure. Heparin is usually unnecessary (level of evidence: B).
2. In patients at high risk of thrombosis, defined as those with any mechanical MV replacement or a mechanical AVR with any risk factor, therapeutic doses of intravenous UFH should be started when the INR falls below 2.0 (typically 48 h before surgery), stopped 4 to 6 h before the procedure, restarted as early after surgery as bleeding stability allows, and continued until the INR is again therapeutic with warfarin therapy (level of evidence: B).
*Risk factors: atrial fibrillation, previous thromboembolism, LV dysfunction, hypercoagulable conditions, older-generation thrombogenic valves, mechanical tricuspid valves, or more than one mechanical valve.
4 ANSWER: D. Please refer to class I recommendations from ACC/AHA 2008 guidelines quoted below for postoperative anticoagulation management following mechanical valve placement.
Class I recommendation:
1. After MV replacement with any mechanical valve, warfarin is indicated to achieve an INR of 2.5 to 3.5 (level of evidence: C).
2. The addition of aspirin 75 to 100 mg once daily to therapeutic warfarin is recommended for all patients with mechanical heart valves and those patients with biological valves who have risk factors* (level of evidence: B).
*Risk factors: atrial fibrillation, previous thromboembolism, LV dysfunction, hypercoagulable conditions, older-generation thrombogenic valves, mechanical tricuspid valves, or more than one mechanical valve.
5 ANSWER: E. Choice E is the one most consistent with the guidelines and is also practical. Class I recommendations are quoted below.
Class I recommendations:
1. Pregnant patients with mechanical prosthetic valves who elect to stop warfarin between weeks 6 and 12 of gestation should receive continuous intravenous UFH, dose-adjusted UFH, or dose-adjusted subcutaneous LMWH (level of evidence: C).
2. For pregnant patients with mechanical prosthetic valves, up to 36 weeks of gestation, the therapeutic choice of continuous intravenous or dose-adjusted subcutaneous UFH, dose-adjusted LMWH, or warfarin should be discussed fully. If continuous intravenous UFH is used, the fetal risk is lower, but the maternal risks of prosthetic valve thrombosis, systemic embolization, infection, osteoporosis, and heparin-induced thrombocytopenia (HIT) are relatively higher (level of evidence: C).
3. In pregnant patients with mechanical prosthetic valves who receive dose-adjusted LMWH, the LMWH should be administered twice daily subcutaneously to maintain the anti-Xa level between 0.7 and 1.2 U per mL 4 h after administration (level of evidence: C).
4. In pregnant patients with mechanical prosthetic valves who receive dose-adjusted UFH, the aPTT should be at least twice control (level of evidence: C).
5. In pregnant patients with mechanical prosthetic valves who receive warfarin, the INR goal should be 3.0 (range 2.5 to 3.5) (level of evidence: C).
6. In pregnant patients with mechanical prosthetic valves, warfarin should be discontinued and continuous intravenous UFH given starting 2 to 3 weeks before planned delivery (level of evidence: C).
6 ANSWER: A. The patient was started on ACE inhibitor (captopril, enalapril, etc.). ACE converts angiotensin I to angiotensin II. It also inactivates bradykinin. ACE inhibitors therefore increase bradykinin levels and decrease angiotensin II levels. Increased bradykinin levels are thought to be responsible for dry cough symptoms in patients taking ACE inhibitors. Digoxin inhibits Na+-K+ ATPase pump. CCBs inhibit calcium entry into vascular smooth muscle cells. Angiotensin II receptor blockers (ARBs) inhibit of activation of angiotensin II receptors. Dry cough is not a recognized side effect of Digoxin, CCBs, or ARBs.
7 ANSWER: C. In the given scenario, atrial fibrillation with pre-excitation is the diagnosis. This is the most likely rhythm with an irregularly irregular wide complex tachycardia in an otherwise healthy patient. In atrial fibrillation with pre-excitation, the patient would be conducting antegrade to the ventricle through both AV node and accessory pathway, and some beats are likely to be fusion beats. Any AV nodal blocking agent (adenosine, digitalis, Diltiazem, β-blocker) is likely to result in unopposed ventricular activation through accessory pathway and can result in ventricular fibrillation. Thus, AV nodal blocking agents are best avoided in this scenario. Amiodarone is a class III antiarrhythmic agent that slows cardiac conduction (including accessory pathway conduction). Direct current cardioversion is the treatment of choice. If this is not possible, amiodarone may be given in this situation as it can restore atrial fibrillation to sinus rhythm as well as decrease accessory pathway conduction.
8 ANSWER: A. The ECG shows sinus rhythm with some conducted p waves as well as frequent nonconducted p waves. Accelerated junctional rhythm is also seen in the first part of the tracing. Of the medications given above, digoxin is the most likely culprit to produce nausea/vomiting and high-grade AV block with activation of ectopic pacemakers (junctional, ventricular, etc.).
9 ANSWER: C. In CPVT patients with VT/VF storm, intravenous β-blocker therapy is considered to be the first-line of treatment. General anesthesia can be used as a last resort if β-blocker therapy is ineffective.
10 ANSWER: C. Since he does not have hemodynamically significant ASD, patient is unlikely to benefit from RSV prophylaxis. He does not meet other criteria for prophylaxis like significant prematurity or coexistent chronic lung condition.
Children who are 24 months of age or younger with hemodynamically significant cyanotic and acyanotic congenital heart disease will benefit from palivizumab prophylaxis
Children younger than 24 months of age with congenital heart disease who are most likely to benefit from immunoprophylaxis include:
• Infants who are receiving medication to control congestive heart failure.
• Infants with moderate to severe pulmonary hypertension.
• Infants with cyanotic heart disease.
11 ANSWER: D. This patient is a candidate for RSV prophylaxis until she is 2 years old. However, the primary benefit of immunoprophylaxis with palivizumab is a decrease in the rate of RSV-associated hospitalization. Results from double-blinded, randomized, placebo-controlled trials with palivizumab involving 2789 infants and children with prematurity, chronic lung disease, or congenital heart disease demonstrated a reduction in RSV hospitalization rates of 39% to 78% in different groups. None of the clinical trials have demonstrated a significant decrease in rate of mortality attributable to RSV infection in infants who receive prophylaxis.
12 ANSWER: A. Furosemide inhibits Na+-2Cl−-K+ cotransporter in the loop of Henle and is therefore termed a loop diuretic. Thiazide diuretics inhibit Na+-Cl− cotransporter. Digoxin inhibits Na+-K+ ATPase pump.
13 ANSWER: D. The patient in the given scenario most likely has idiopathic/viral pericarditis. Ibuprofen or aspirin has been most commonly used and provides prompt relief of pain in most patients but does not alter the natural history of the disease. High-dose aspirin (800 mg orally every 6 to 8 hours for 7 to 10 days followed by gradual tapering of the dose by 800 mg per week for 3 additional weeks) is usually recommended if aspirin is used. Although acute pericarditis appears to respond dramatically to corticosteroids, early use of corticosteroids has been associated with an increased risk of relapsing pericarditis in multiple studies.
Routine use of colchicine in the treatment of acute pericarditis has been supported by the Colchicine for acute pericarditis (COPE) trial that randomized patients into receiving aspirin alone versus aspirin + colchicine. A 4-to-6-week Colchicine therapy may be considered in patients with acute pericarditis, especially in those who have not benefitted from NSAID therapy after 1 week. In this given scenario, ibuprofen is the best option given the side effect profile of colchicines, and colchicine would require a longer course than listed.
14 ANSWER: B. NIRS saturation is a good surrogate for tissue level saturation/oxygenation. NIRS saturation can be substituted for a mixed venous saturation (MVO2). The difference between SaO2 and MVO2 is a surrogate for cardiac output that is likely to be low given the difference of 40 (80 – 40) in this scenario, which would explain the pH of 7.2 (acidosis).
The pulmonary venous O2 can be assumed to be close to 100% given the FiO2 of 21% and clear lungs. The patients Qp/Qs in this scenario would around 2.
Qp/Qs= (SaO2 – MVO2)/(Pulmonary venous O2 – SaO2) = (80 – 40)/(100 – 80) = 40/20= 2.
Thus, patient has a low systemic cardiac output state and his lungs are getting at least 2 times the systemic blood flow. Norepinephrine is a potent vasoconstrictor. Weaning norepinephrine would lower systemic vascular resistance (SVR) and improve cardiac output, making the Qp/QS more balanced. This should be the first line of management in addition to giving fluids that has already been tried in this patient. IV furosemide would decrease the intravascular volume and be detrimental for the patient. IV β-blocker therapy may decrease cardiac inotropy and worsen the low output state. Decreasing the milrinone would reduce the systemic cardiac output by increasing the SVR and by decreasing the cardiac inotropy. Increasing the FiO2 would lower the PVR and lead to more pulmonary blood flow at the expense of systemic blood flow (increase in Qp/Qs).
15 ANSWER: E. Answer e is most appropriate indication for IV steroids in KD. Initial therapy for KD during the acute phase is IVIG and high-dose aspirin. In case of persistence or recurrence of fever despite one dose of IVIG, another dose should be repeated. For children who defervesce with a second IVIG infusion, but in whom fever recurs, a third dose of IVIG or alternately intravenous steroids (methylprednisolone) may be considered. Oral steroids would not be appropriate therapy for KD.
16 ANSWER: C. The patient has mild to moderate carditis that needs therapy with high-dose aspirin (80 to 100 mg/kg/day in four divided doses in children). Oral prednisone is indicated for more severe carditis associated with a sicker patient in the setting of heart failure, severe valvular regurgitation, significant pericarditis/myocarditis, or reduced cardiac function. There is no recommendation for combing oral steroids with aspirin for treatment of acute RF. IVIG + aspirin is used in the treatment of KD. There is no indication for a β-blocker in pericarditis.
17 ANSWER: C. Sirolimus acts at a more distal site in the lymphocyte activation cascade by blocking transcription of activation genes. Sirolimus (also known as rapamycin) is not a calcineurin inhibitor, but tacrolimus and cyclosporine are. Cyclosporine and tacrolimus are calcineurin inhibitors. Cyclosporine and tacrolimus are available for intravenous use. Tacrolimus offers no survival advantage over cyclosporine in heart transplant recipients. Sirolimus may be less nephrotoxic over the long term.
18 ANSWER: C. Patient had mild carditis during RF, but is free of residual heart disease now. Per guidelines, she will need RF antibiotic prophylaxis for at least 10 years or until 21 years of age, whichever is longer.
As per the current guidelines,
I. RF patients with carditis and residual heart disease (persistent valvular disease) should receive treatment for a duration of 10 years or until 40 years of age (whichever is longer, sometimes lifelong) after the last attack of RF.
II. RF patients with carditis but without residual heart disease (no valvular disease) should receive treatment for a duration of 10 years or until 21 years of age (whichever is longer) after the last attack of RF.
III. RF patients without carditis should receive treatment for a duration of 5 years or until 21 years of age (whichever is longer) after the last attack of RF.
19 ANSWER: E. Please refer to guidelines as quoted below.
Class IIa recommendations:
Prophylaxis against IE is reasonable for the following patients at highest risk for adverse outcomes from IE who undergo dental procedures that involve manipulation of either gingival tissue or the periapical region of teeth or perforation of the oral mucosa:
• Patients with prosthetic cardiac valves or prosthetic material used for cardiac valve repair (level of evidence: B).
• Patients with previous IE (level of evidence: B).
• Patients with CHD (level of evidence: B).
 Unrepaired cyanotic CHD, including palliative shunts and conduits (level of evidence: B).
Unrepaired cyanotic CHD, including palliative shunts and conduits (level of evidence: B).
 Completely repaired congenital heart defect repaired with prosthetic material or device, whether placed by surgery or by catheter intervention, during the first 6 months after the procedure (level of evidence: B).
Completely repaired congenital heart defect repaired with prosthetic material or device, whether placed by surgery or by catheter intervention, during the first 6 months after the procedure (level of evidence: B).
 Repaired CHD with residual defects at the site or adjacent to the site of a prosthetic patch or prosthetic device (both of which inhibit endothelialization) (level of evidence: B).
Repaired CHD with residual defects at the site or adjacent to the site of a prosthetic patch or prosthetic device (both of which inhibit endothelialization) (level of evidence: B).
• Cardiac transplant recipients with valve regurgitation due to a structurally abnormal valve (level of evidence: C).
IE prophylaxis is no longer recommended for the following dental procedures: routine anesthetic injections through noninfected tissue, dental radiographs, placement/removal of orthodontic/prosthodontic appliances, shedding of deciduous teeth, and bleeding from trauma to lips/oral mucosa.
20 ANSWER: B. The child is ≥10 years old and meets criteria for pharmacological lipid lowering therapy as per guidelines quoted below. His risk factors include male sex, obesity, low HDL, and high triglycerides. For children meeting criteria for starting lipid-lowering drug therapy, a statin is recommended as first-line treatment.
Recommendations for drug therapy of high-risk hyperlipidemia in children and adolescents original recommendations of the NCEP Expert Panel:
1. Consider drug therapy in children ≥10 years of age (usually wait until menarche for females) and after a 6- to-12-month trial of fat- and cholesterol-restricted dietary management.
2. Consider drug therapy if LDL level remains ≥4.90 mmol/L (190 mg/dL) or LDL remains ≥4.10 mmol/L (160 mg/dL) and
a. there is a positive family history of premature cardiovascular disease.
b. ≥2 other risk factors are present in the child or adolescent after vigorous attempts to control these risk factors.
Risk factors and high-risk conditions may include male gender, strong family history of premature cardiovascular disease or events, presence of associated low HDL, high triglycerides, small dense LDL, presence of overweight or obesity and aspects of the metabolic syndrome, presence of other medical conditions associated with an increased atherosclerotic risk such as diabetes, HIV infection, systemic lupus erythematosus, organ transplantation, survivors of childhood cancer, presence of hypertension, current smoking, and passive smoke exposure and presence of novel and emerging risk factors and markers, for example, elevated lipoprotein(a), homocysteine, C-reactive protein.
Encouraging results have been obtained from clinical trials of statins in children and adolescents with familial or severe hypercholesterolemia. Adverse effects do not appear to be increased over those noted in clinical studies in adults; however, ultra-long-term safety and compliance remain of concern, as does demonstration of an impact on clinical disease. Lovastatin, simvastatin, pravastatin, and atorvastatin have pediatric labeling from the US Food and Drug Administration on the basis of clinical trials performed in children with familial hypercholesterolemia.
Given the high prevalence of high gastrointestinal complaints, poor palatability, low compliance, and limited effectiveness, it is unlikely that the bile acid–binding resins will be sufficient to achieve target LDL cholesterol levels in children who meet the criteria for lipid-lowering drug therapy.
Fibric acid derivatives should be used preferentially for children with severe elevations in triglyceride levels who are at risk for pancreatitis.
Given the reported poor tolerance, the potential for very serious adverse effects, and the limited available data, niacin cannot be routinely recommended for children who need treatment for hypercholesterolemia but may be considered for selected patients.
21 ANSWER: D. Patient needs treatment because of symptoms with exertion. The best therapeutic option is medication alone and a β-blocker is generally preferred. If CCBs are used, then preferred medications would be diltiazem and verapamil. Dihydropyridine CCBs like Nifedipine would cause peripheral vasodilatation and reflex tachycardia that are both detrimental in a HCM patient with obstruction. Furosemide by reducing preload and therefore left ventricular filling (through its diuretic effect) could worsen the degree of obstruction in a HCM patient. Invasive intervention (myectomy/septal ablation) for LVOT gradient >50 mm Hg is only recommended for symptomatic patients refractory to medical therapy. ICD is not indicated at present as the patient has no clear sudden death risk factors.
22 ANSWER: B. Sirolimus can inhibit smooth muscle proliferation and may have the advantage of inhibiting coronary vasculopathy. Sirolimus is not a calcineurin inhibitor and is most often used in combination with a calcineurin inhibitor (cyclosporine, tacrolimus). It may also be considered in lieu of calcineurin inhibitors. Sirolimus may also less nephrotoxic over the long term.
23 ANSWER: A. Anesthetic drugs alone cannot fully eliminate the stress response associated with profound hypothermia. Phenoxybenzamine is a long-acting irreversible α-adrenergic blocker that reduces SVR and may be useful in this setting, although hypotension and hypoperfusion may result. SVR is elevated and results in an unfavorable Qp/Qs ratio with reduced systemic blood flow and low cardiac output state. Phenoxybenzamine is useful to ameliorate this stress-induced SVR response. Milrinone, nitroprusside, and dobutamine also have vasodilatory properties and can be useful adjuncts in reducing SVR. Norepinephrine on the other hand causes systemic vasoconstriction and elevates SVR. Dopamine, epinephrine, and clonidine would not be very useful in reducing the elevated SVR in this setting.
24 ANSWER: B. Fentanyl, pancuronium, and ketamine (if needed) are ideal drugs in this situation. Narcotics like fentanyl and sufentanil given slowly provide better hemodynamic stability in conjunction with neuromuscular blocking agent pancuronium. Succinylcholine is a depolarizing neuromuscular blocking agent and should be avoided in children with cardiovascular compromise. Pancuronium is a nondepolarizing neuromuscular blocking agent. Dosage requirements of pancuronium are unchanged in children with congenital heart disease or intracardiac shunts. Thiopental can produce myocardial depression and therefore not preferred in sedating cardiac patients. Pancuronium produces no significant HR or BP changes when given slowly. A bolus dose of pancuronium can produce tachycardia and hypertension through its sympathomimetic effect that may be desirable in this situation (low cardiac output state). Ejection fraction of children with CHD is typically well preserved after ketamine. Ketamine should be typically used in conjunction with atropine.
25 ANSWER: E. Both adenosine and β-blockers have the potential to exacerbate bronchospasm in this patient. Although the electrophysiologic effects of adenosine are temporary, the bronchospasm may persist for a long period of time. Heart transplant recipients are particularly sensitive to adenosine, and one-quarter to one-half the dose should be used initially as long periods of AV block may be noted with higher doses. Adenosine has a half life of <2 s and is metabolized quickly in the blood. It therefore must be given as rapidly as possible in a large-bore IV as close to the heart as possible. Flushing and hypotension are common side effects. The bradycardia caused by adenosine may precipitate other arrhythmias including atrial fibrillation or ventricular tachycardia, so an external defibrillator should be readily available. The typical dose is 100 to 400 μg/kg in children.
26 ANSWER: C. Ambrisentan is a newer, selective endothelin A receptor antagonist. It does not induce or inhibit cytochrome P450 enzymes and is metabolized through glucuronidation. Therefore it is much less hepatotoxic than bosentan. Epoprostenol is a prostacyclin (PGI2) analogue and is not a prostaglandin (PGE2) analogue. Sildenafil works through nitric oxide-cyclic GMP cascade, but it is a phosphodiesterase 5 inhibitor and not a phosphodiesterase 3 inhibitor. Milrinone is a phosphodiesterase 3 inhibitor. Combination therapy is increasingly used in children to treat severe pulmonary arterial hypertension despite the lack of published evidence. However, there are studies published on combination therapy in adult patients with pulmonary arterial hypertension.
27 ANSWER: D. The ECG changes in Brugada syndrome can be dynamic and thus missed on a single ECG screening. Since the characteristic ECG hallmark may be concealed, drug challenge with sodium channel blockers (which may exacerbate the sodium channel dysfunction) to bring out the typical ECG changes has been proposed as a useful tool for the diagnosis of Brugada syndrome. Drugs employed for this purpose have included ajmaline, flecainide, procainamide, pilsicainide, disopyramide, and propafenone although the specific diagnostic value for all of them has not yet been systematically studied. Epinephrine challenge is helpful in identifying concealed LQTS. Cardiac MRI may be used in the diagnosis of patients with arrhythmogenic right ventricular cardiomyopathy. Isoproterenol testing is commonly used in the EP lab to bring out arrhythmias. Exercise testing may be helpful in the diagnosis of CPVT.
28 ANSWER: D. Phenytoin, lidocaine, and mexiletine are all class IB antiarrhythmic sodium channel blocking drugs characterized by rapid recovery of the blocked sodium channel. QT intervals may be slightly shortened by these drugs. There is no contraindication to phenytoin use in LQTS patients. There is at present no role for IV β-blocker or amiodarone in the absence of any significant ventricular ectopy. Class III agents like amiodarone, sotalol, and ibutilide block the potassium channels and prolong the QTc interval.
29 ANSWER: B. The patient is symptomatic with atrial flutter but is hemodynamically stable. Therefore, the priority of the physician is to treat her symptoms using medication(s). Electrical cardioversion is not the first-line treatment for a stable patient. Of the medications given, IV diltiazem is the best option as it would slow down the rapid ventricular response and can produce symptomatic relief. IV β-blockers and sotalol are other options. IV digoxin is preferred less these days for such situations. Class IC antiarrhythmic agent flecainide can slow down the atrial conduction within the flutter circuit and therefore slow down flutter rate. Thus it can convert fast flutters with AV block into slow flutters with 1:1 AV conduction if administered alone. Class I antiarrhythmic agent disopyramide has anti-cholinergic activity and may enhance AV node conduction and worsen the situation when administered alone. Therefore drugs like flecainide and disopyramide are best administered in conjunction with an AV nodal blocking agent. IV labetalol is a nonselective β-blocker and is primarily used in hypertensive emergencies.
30 ANSWER: C. Levosimendan is a calcium-sensitizing agent that binds to Troponin C and improves contractile efficiency as well as reduces afterload. Verapamil is an “L” type CCB and reduces intracellular calcium by reducing calcium-induced calcium release. Digoxin is a Na-K ATPase inhibitor and indirectly increases intracellular calcium. Milrinone is a phosphodiesterase 3 inhibitor. Nesiritide is a synthetic BNP used to treat decompensated heart failure patients.
31 ANSWER: D. Isoproterenol stimulates myocardial β-1 receptors resulting in positive chronotropy and inotropy. It can result in the generation of a stable junctional/ventricular escape rhythm that is helpful in this setting allowing for additional time to pursue interventions like temporary pacemaker if necessary. Atropine is anti-cholinergic/vagolytic agent and only works in reversing AV block to excessive vagal effect. It would not be helpful in this situation. Milrinone and dobutamine do not have the same effect as isoproterenol and therefore are not indicated. Digoxin may slow the junctional rate and therefore is not indicated.
32 ANSWER: A. The patient has low cardiac output despite a EF of 70% because a significant fraction of the left ventricular stroke volume can be expected to leak into the left atrium (LA) resulting in reduced forward systemic stroke volume. Elevated left atrial pressure can be expected and would result in pulmonary edema. She would benefit the most from a systemic vasodilator like nitroprusside that would increase her forward stroke volume and improve her cardiac output. IV furosemide would help by reducing pulmonary edema, but not primarily by improving forward stroke volume. Vasopressin is a vasoconstrictor and would be detrimental in this situation. Digoxin would not helpful as the patient does not have myocardial dysfunction or reduced EF. Dopamine is not a systemic vasodilator and would not improve the patient’s hemodynamics.
33 ANSWER: C. The given clinical scenario does not suggest a TOF spell. Since the RVOT murmur is still loud and the patient is alert, he is unlikely to be in any acute RVOT obstructive crisis. The patient’s hematocrit is only 26, which is low for an unrepaired TOF patient. The low oxygen carrying capacity in the setting of an underlying cyanotic heart disease could result in reduced activity levels.
Anemia could cause a drop in the SpO2 in the following ways. Systemic vasodilation associated with anemia may shift blood flow from the lungs to the systemic circulation. Thus, there would be more right-to-left shunting as SVR drops causing a drop in SpO2. Also in the setting of a low hemoglobin, tissue oxygen extraction would result in a much lower mixed venous saturation than compared to somebody with higher hemoglobin levels. In the absence of any right-to-left shunt, all this blood would be fully oxygenated in the lungs. But in the presence of a right-to-left shunt, a proportion of this blood (with lower mixed venous SpO2) would mix with the oxygenated blood resulting in a much lower systemic SpO2.
Since the patient is hypoxic and symptomatic treatment is indicated. Of the following options, blood transfusion would benefit the patient in the ER setting. It would increase his oxygen carrying capacity and could also improve his SpO2 for the above-mentioned reasons. Intravenous propranolol, phenylephrine infusion, and morphine administration are useful in patients who have a TOF spell that is not the case here. Furosemide therapy would not be helpful as pulmonary overcirculation is rare in TOF.
34 ANSWER: E. Acute side effects of PGE1 include apnea (needing intubation), fever/hyperthermia, hypotension, and seizures. Cutaneous vasodilation and edema can develop. In patients who have been kept on long-term PGE1 therapy (beyond 2 weeks), various side effects including cortical hyperostosis has been described.
35 ANSWER: A. Losartan is an angiotensin receptor 1 (AT1R) antagonist and has been shown to antagonize TGF-β signaling. The exact mechanism of action is uncertain, but activation of angiotensin type 1 receptors increases the expression of TGF-β ligands and receptors and induces the activation of thrombospondin, a powerful TGF-β activator. Propranolol, enalapril, verapamil, or spironolactone does not have the above effect.
36 ANSWER: D. Eplerenone is a newer mineralocorticoid receptor (aldosterone receptor) antagonist. Most of its effects are like spironolactone (including hyperkalemia). Enalapril and captopril both increase potassium levels. Metoprolol has no effect on potassium levels.
37 ANSWER: C. Amiodarone increases the levels of cyclosporine, digoxin and warfarin (increased anticoagulant effect) by inhibiting the activity of cytochrome P450. In the setting of pre-existent β-blocker therapy as in this patient there is potential for heart block (not enhanced AV nodal conduction) due to the AV nodal blocking effect of amiodarone. There is no interaction requiring dose adjustment with steroids and amiodarone.
38 ANSWER: B. Amiodarone (class III antiarrhythmic agent) is primarily a cardiac potassium channel blocker. It prolongs repolarization and therefore QTc interval. However, it is also a broad spectrum antiarrhythmic agent and blocks cardiac sodium and sodium channels as well. It produces β-blockade, causes reduced AV nodal conduction, and is not a vagolytic agent. Hypokalemia exacerbates the pro-arrhythmic potential of amiodarone and can precipitate torsades de pointes.
39 ANSWER: C. It is true that tacrolimus recipients (8%) more often develop diabetes mellitus than cyclosporine recipients (2%). Tacrolimus levels, HLA-DR mismatch and older age at transplantation may predispose to posttransplant diabetes. Sirolimus use is associated with bone marrow suppression, especially when used in conjunction with tacrolimus. Lipid abnormalities are common even in younger children who are heart transplant recipients, and lipid-lowering therapy is often instituted in this sub-group. CCB and ACE inhibitors are typically used for managing hypertension in pediatric heart transplant recipients. Sirolimus is less nephrotoxic than cyclosporine or tacrolimus.
40 ANSWER: C. Drugs that lower PVR include tolazoline (a nonselective competitive α-adrenergic receptor antagonist), nitric oxide (not nitrous oxide), dobutamine (not dopamine), milrinone, prostaglandins, prostacyclins, sodium nitroprusside, and sildenafil. Ketamine may increase PVR. Norepinephrine is a systemic vasoconstrictor and is not a pulmonary vasodilator.
41 ANSWER: D. The patient in the given scenario is likely to have heparin-induced thrombocytopenia with thrombosis syndrome (HITTS) that develops in a subset of patients with HIT. Heparin combines with platelet factor 4 (PF-4) complex and makes it immunogenic. The resulting antibodies to this complex may result in the formation of platelet aggregates (which can cause vaso-occlusion) and cause immune-mediated platelet destruction resulting in thrombocytopenia (usually a >50% drop in platelet count). Diagnosis is made using specific antibody assay. However, once thrombotic complication is noted in the setting of suspected HIT, urgent medical therapy is indicated. The best course of action is to completely stop the heparin altogether and provide immediate alternative anticoagulation medications.
The degree of platelet drop in HIT patients is not enough to cause clinically significant bleeding and therefore platelet transfusion is not indicated. Low-molecular-weight heparins (like enoxaparin), although may not provoke HIT, may still cross-react with heparin antibodies and may not be safe in HIT patients.
42 ANSWER: C. Use of warfarin during pregnancy is associated with various teratogenic side effects including defects in calcification of the epiphyses (chondrodysplasia punctata), retarded intrauterine growth, psychomotor deficit, hypotonia, convulsions, nasal hypoplasia, ocular and CNS anomalies. Risk is higher during the first trimester (~10%), and the critical period is between the 6th and 9th week of gestation. The risk is estimated ~3% to 5% for administration during the second and third trimesters. Lithium has been associated with Ebstein’s anomaly and not left-sided obstructive lesions. Amiodarone can cause hypothyroidism or hyperthyroidism, but complete heart block is not a typical finding and it is not permanent. ACE inhibitors can cause renal damage, cranial ossification defects, oligohydramnios, and delayed intra-uterine growth, but right-sided obstructive lesions have not been described. They are contraindicated during pregnancy, especially the second and third trimesters. High-dose folic acid therapy is known to be protective against neural tube defects.
43 ANSWER: E. The patient has serious digoxin toxicity and is symptomatic (dizziness and mild hypotension) with high-grade AV block. He also has significant ventricular ectopy including nonsustained VT.
Intravenous atropine and temporary pacing are recommended in such patients with high-degree symptomatic AV block. Digoxin antibody Fab should be administered in patients showing serious signs of digoxin toxicity (symptomatic AV block, serious ventricular arrhythmias), and this patient would be a candidate.
Concomitant therapy with agents such as activated charcoal and cholestyramine have also been recommend in patients showing serious digoxin toxicity in an attempt to bind digoxin in the gut. Such agents facilitate gastrointestinal elimination as well as increase the systemic clearance of digoxin. Through both passive diffusion and enterohepatic recycling of digoxin, the intestine acts as a dialysis membrane, and the binding of the charcoal resin aids in the elimination of digoxin.
Digoxin is 50% to 70% eliminated through the kidneys unmetabolized without significant hepatic contribution, and therefore, liver dysfunction (due to recent infectious mononucleosis) is not the direct reason for elevated digoxin levels. In the setting of preexisting renal dysfunction, reduced oral intake following the viral illness could have contributed to exacerbated renal dysfunction (pre-renal etiology) and associated hyperkalemia. This could result in reduced renal excretion of digoxin and precipitate digoxin toxicity. Hyperkalemia exacerbates digoxin toxicity and concurrent treatment of hyperkalemia would be beneficial, although the potassium level would not give the definitive cause of the AV block, and the QRS is not widened and the t waves are not peaked so the level is likely not severely elevated.
This patient needs the following management: IV fluids to improve renal perfusion and hypotension, treatment of hyperkalemia, IV atropine acutely (temporary pacing is also indicated), digoxin antibody therapy, and management of renal dysfunction. Intravenous lidocaine can be administered if the patient develops symptomatic ventricular arrhythmias before digoxin antibody becomes available.
44 ANSWER: B. The patient has persistent postoperative hypertension that is significant, and in an intubated patient, it is not easy to evaluate symptoms. She should be treated for hypertension. She has a history of persistent asthma as judged by her medication list, and intravenous labetalol (β-blocker) can exacerbate bronchoconstriction and worsen her hypoxia. In the setting of concurrent renal and hepatic dysfunction, sodium nitroprusside is not safe due to potential buildup of cyanide. Nicardipine is a CCB and can be used in situations where β-blocker and sodium nitroprusside are contraindicated. It does not have any adverse effects on the myocardium.
Patient’s hypoxia is most likely due to atelectasis, and since there is no mention of pulmonary hypertension, there is no role for nitric oxide therapy. Dexmedetomidine is a highly selective α-2 receptor agonist and is used for sedation. It can produce dose-dependent decreases in BP and HR as a result of its α-2 agonist effect on the sympathetic ganglia with resulting sympatholytic effects. However, it is not indicated in the current scenario as the patient seems to be well sedated already.
45 ANSWER: D. The above clinical scenario is consistent with a “suicidal right ventricle” due to persistent dynamic infundibular/subpulmonary obstruction that can follow acute relief of a distal fixed pulmonary valve obstruction. The severe subvalvular obstruction in the absence of a distal fixed obstruction can result in complete/near complete RVOT obstruction. This can lead to acute right ventricular failure with poor RV filling and right-to-left shunt through the patent foramen ovale. Intravenous β-blockers would be the drug of choice as they can relieve the dynamic RVOT obstruction and improve the hemodynamics. There is no role for pulmonary vasodilators like nitric oxide in this setting. Milrinone is an inotrope and can worsen the dynamic obstruction. Phenylephrine is a vasoconstrictor and is unlikely to produce any beneficial hemodynamic effects in this scenario. Intravenous diuretics like furosemide have no specific role in this situation. In fact it may reduce right ventricular preload and worsen the condition.
46 ANSWER: B. Very rarely, statins can cause life-threatening rhabdomyolysis. The most common symptom is muscle pain. Creatine kinase levels should be checked to rule out this condition. Rhabdomyolysis can cause severe muscle pain, liver damage, kidney failure, and death. Other side effects include diarrhea, liver damage, gastrointestinal problems such as diarrhea or nausea, rash and flushing, and neurological side effects.
47 ANSWER: A. As a diuretic, chlorothiazide inhibits active chloride reabsorption at the early distal tubule through the Na-Cl cotransporter, resulting in an increase in the excretion of sodium, chloride, and water.
48 ANSWER: C. Furosemide is a loop diuretic. It acts by inhibiting the Na+– K+-Cl− cotransporter in the thick ascending limb of the loop of Henle. It also interferes with the reabsorption of K +, Ca++, and Mg++ and may therefore be helpful in patients with hypercalcemia. It may cause kidney stones, particularly in high doses.
49 ANSWER: B. Acetazolamide is an enzyme inhibitor that acts specifically on carbonic anhydrase. The diuretic effect of acetazolamide is due to its action in the kidney on the reversible reaction involving hydration of carbon dioxide and dehydration of carbonic acid. This results in the renal loss of HCO3, sodium, water, and potassium. Alkalinization of the urine and promotion of diuresis result from this process.
50 ANSWER: E. Metolazone has properties generally similar to the thiazide diuretics. The actions of metolazone result from interference with electrolyte reabsorption. Metolazone acts primarily to inhibit sodium reabsorption at the cortical diluting site and to a lesser extent in the proximal convoluted tubule. Sodium and chloride ions are excreted in approximately equivalent amounts. The increased delivery of sodium to the distal tubular exchange site results in increased potassium excretion. Metolazone may be used to augment the function of loop diuretics.
SUGGESTED READINGS
American Academy of Pediatrics Subcommittee on Diagnosis and Management of Bronchiolitis. Diagnosis and management of bronchiolitis. Pediatrics. 2006;118:1774–1793 (pp. 1784–1785).
Bauman JL, Didomenico RJ, Galanter WL. Mechanisms, manifestations, and management of digoxin toxicity in the modern era. Am J Cardiovasc Drugs. 2006;6:77–86.
Beekman RH, Tuuri DT. Acute hemodynamic effects of increasing hemoglobin concentration in children with a right to left ventricular shunt and relative anemia. J Am Coll Cardiol. 1985;5(2 Pt 1):357–362.
Bonow RO, Carabello BA, Chatterjee K, et al. 2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease…. J Am Coll Cardiol. 2008;52:e1–e142 (p. e104).
Cardiac intensive care (Chapter 20). In: Moss and Adams: 448–480
(p. 457).
Clin Cardiol. 2008;3:153–158.
Constantine E, Linakis J. The assessment and management of hypertensive emergencies and urgencies in children. Pediatr Emerg Care. 2005;21:391–396.
De Santis M, Straface G, Carducci B, et al. Risk of drug-induced congenital defects. Eur J Obstet Gynecol Reprod Biol. 2004;117:
10–19.
Dilated congestive cardiomyopathy (Chapter 57). In: Moss and Adams: 1195–1205 (p. 1204).
Disorders of cardiac rhythm and conduction (Chapter 14). In: Moss and Adams: 293–342.
Drew BJ, Ackerman MJ, Funk M, et al. Prevention of torsades de pointes in hospital settings: a scientific statement from the American Heart Association and the American College of Cardiology Foundation. Circulation. 2010;121:1047–1060 (p. 1052).
Epidemiology and prevention of congenital heart defects (Chapter 25). In: Moss and Adams: 524–545.
Gersh BJ, Maron BJ, Bonow RO, et al. 2011 ACCF/AHA Guideline for the diagnosis and treatment of hypertrophic cardiomyopathy. Circulation. 2011;124:37–85 (p. 54).
Gerber MA, Baltimore RS, Eaton CB, et al. Prevention of rheumatic fever and diagnosis and treatment of acute Streptococcal pharyngitis: a scientific statement from the American Heart Association Rheumatic Fever…. Circulation. 2009;119:1541–1551 (p. 1547).
Hypoplastic left heart syndrome (Chapter 50). In: Moss and Adams: 1005–1038 (pp. 1016, 1017, 1023).
Kawasaki disease (Chapter 61). In: Moss and Adams: 1242–1256 (p. 1251).
Khandaker MH, Espinosa RE, Nishimura RA, et al. Pericardial disease: diagnosis and management. Mayo Clin Proc. 2010;85(6):572–593 (pp. 577–578).
Lewis AB, Freed MD, Heymann MA, et al. Side effects of therapy with prostaglandin E1 in infants with critical congenital heart disease. Circulation. 1981;64:893–898.
Mason KP. Sedation trends in the 21st century: the transition to dexmedetomidine for radiological imaging studies. Paediatr Anaesth. 2010;20:265–272.
McCrindle BW, Urbina EM, Dennison BA, et al. Drug therapy of high-risk lipid abnormalities in children and adolescents: a scientific statement from the American Heart Association Atherosclerosis, Hypertension, and Obesity in Youth Committee, Council of Cardiovascular Disease in the Young, with the Council on Cardiovascular Nursing. Circulation. 2007;115:1948–1967 (p. 1962).
Nishimura RA, Carabello BA, Faxon DP, et al. ACC/AHA 2008 guideline update on valvular heart disease: focused update on infective endocarditis: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines: endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation. 2008;118:887–896 (pp. 892, 893).
Oishi P, Datar SA, Fineman JR. Pediatric pulmonary arterial hypertension: current and emerging therapeutic options. Expert Opin Pharmacother. 2011;12:1845–1864.
Pediatric heart transplantation (Chapter 18). In: Moss and Adams: 426–438 (p. 431).
Pediatric heart transplantation (Chapter 18). In: Moss and Adams: 426–438.
Prog Cardiovasc Dis. 2008;5:1–22.
Pulmonary stenosis (Chapter 40). In: Moss and Adams: 835–859 (p. 845).
Reddy SC, Saxena A. Prostaglandin E1: first stage palliation in neonates with congenital cardiac defects. Indian J Pediatr. 1998;65:211–216.
Rheumatic fever and rheumatic heart disease (Chapter 62). In: Moss and Adams: 1256–1280 (p. 1271).
Tálosi G, Katona M, Túri S. Side-effects of long-term prostaglan-
din E(1) treatment in neonates. Pediatr Int. 2007; 49:335–340.
Tetralogy of Fallot (Chapter 43). In: Moss and Adams: 888–921.
Trujillo TC, Nolan PE. Antiarrhythmic agents: drug interactions of clinical significance. Drug Saf. 2000;23:509–532.
Williams A, Davies S, Stuart AG, et al. Medical treatment of Marfan syndrome: a time for change. Heart. 2008;94:414–421.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


