TABLE 181.1 Symptoms at Presentation | ||||
|---|---|---|---|---|
|
syndromic context. Those tumors occurring in the setting of CNC have a relatively high rate of recurrence (10% to 20%), while those outside of CNC have a very low recurrence rate (<5%).17,18 Most recurrences occurring in nonsyndromic tumors occur as a result of incomplete tumor resection, which is why it is recommended that the cardiac surgeon take a rim of normal tissue at the attachment site to ensure complete excision.
TABLE 181.2 Diagnostic Criteria for Carney Complexa | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||
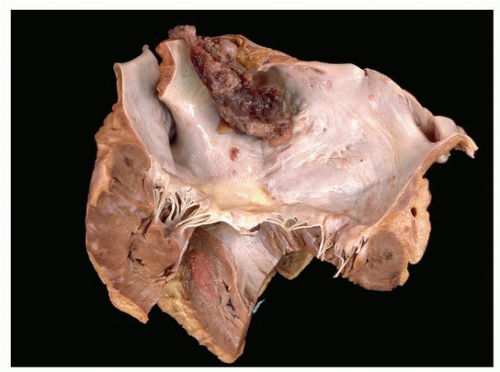 FIGURE 181.1 ▲ Left atrial cardiac myxoma arising from the septum. The sizeable tumor is protruding into the left atrial cavity and partially obstructed blood flow through the mitral valve. |
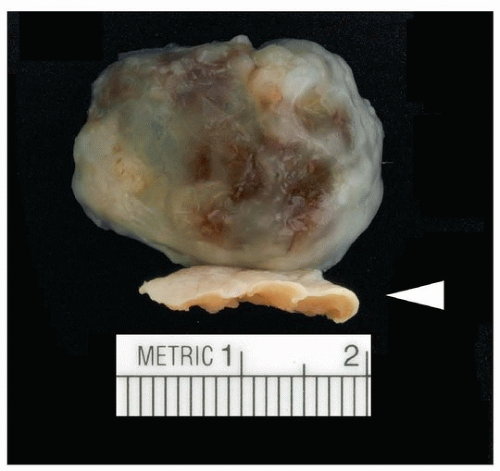 FIGURE 181.2 ▲ Cardiac myxoma with endocardial attachment (arrowhead). A rim of the myocardium is typically taken with the tumor at surgical resection to ensure completeness of excision. |
 FIGURE 181.3 ▲ A smooth surface tumor with a relatively broad base (bottom). |
thromboembolic symptoms, either from adherent surface thrombus on the finger-like projections of tumor or from the friable tumor itself.19
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


