Chapter 5 Cardiac masses, pericardial disease and myocarditis
Cardiac masses
The general protocol for interrogation and subsequent reporting of masses is:
Thrombus
This is by far the commonest cardiac filling defect and both atrial and ventricular thrombi are readily visualized by SE, GE and following gadolinium (Figure 5.1). On T1W SE imaging, thrombus has intermediate signal intensity often slightly higher than myocardium and blood. T2W SE shows surrounding slow-flowing blood as having higher signal intensity than the thrombus itself, thereby enhancing differentiation from myocardium. With SSFP cine GE and velocity mapping techniques thrombus has the lowest signal intensity in distinction to blood flow, even where it is diminished, which has a high signal intensity. Injection of gadolinium contrast agent increases diagnostic accuracy and characteristically demonstrates an avascular filling defect by rest perfusion CMR and EGE. In the case of LV thrombus, subsequent LGE images usually reveal an area of infarction which has acted as the substrate for thrombus formation. For atrial thrombi, a dilated LA and LA appendage can be demonstrated as with transoesophageal echocardiography (TOE).
Tumours
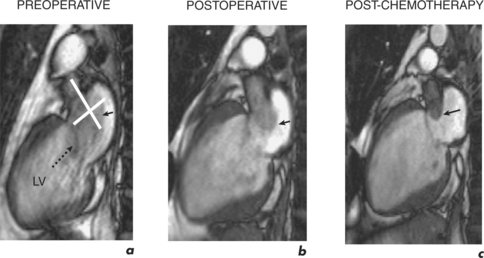
Secondary cardiac deposits are more frequent than primary cardiac tumours, but both are rare with a necropsy incidence of 1% and 0.05% respectively. Secondary involvement is usually clinically silent and limited to the epicardium. Presenting cardiac signs, when they occur, are those of a large pericardial effusion or incipient tamponade, arrhythmias, cardiomegaly or heart failure. Locally infiltrating malignancies include carcinoma of the lung or breast and renal cell carcinoma may embolize to the RA (Figure 5.2). Cardiac metastases are seen with malignant melanomas, leukaemias and lymphomas.

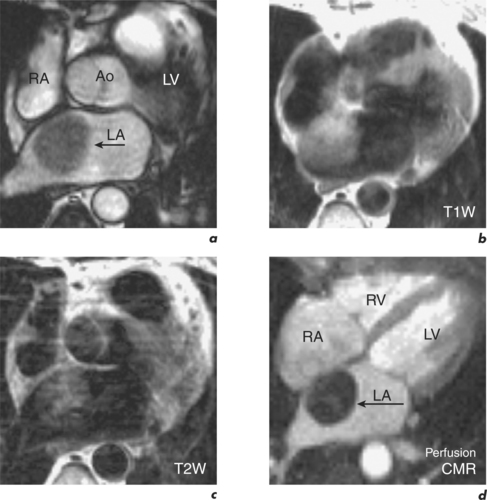
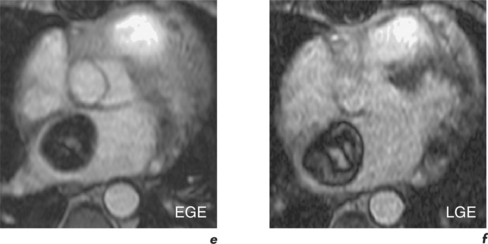
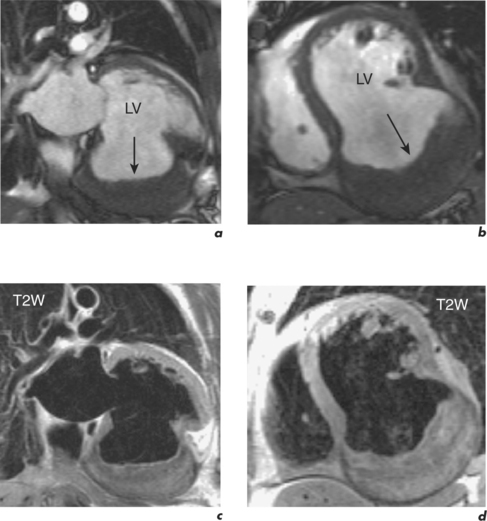
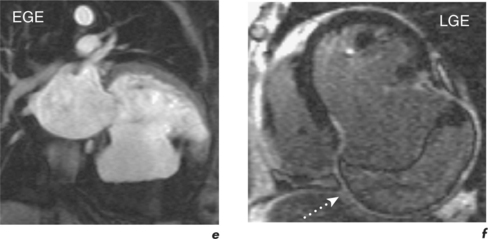
The majority of primary cardiac tumours are benign with the most frequent being atrial myxomas (45%) and cardiac lipomas (20%) (Figure 5.3). Malignant cardiac tumours make up one quarter of primary tumours and the most common are sarcomas (95%). CMR anatomical evaluation of intra- and extracardiac involvement has implications for staging, surgical treatment and surveillance (Figure 5.4). CMR differentiation between malignant and benign tumours uses a combination of general principles applied by other modalities and some more specific features. In general terms, malignancy is more likely with larger masses having a broad-based attachment, involving more than one cardiac chamber or great vessel, and with associated pericardial or extracardiac extension. More specifically, T1W and T2W images use the biochemical composition of masses to assist with diagnosis. High signal intensity on T1W images can be due to cystic lesions with a high protein content, fatty tumours (lipoma, liposarcoma), recent haemorrhage and melanoma. Low signal intensity on T1W is seen in cysts with low protein content, within vascular malformations, in calcified lesions, or if the mass contains air. Subsequent T2W imaging demonstrates cysts as having high signal intensity, and the addition of a fat saturation prepulse distinguishes lipid content. Rest perfusion first-pass CMR shows contrast uptake into vascular tumours (haemangioma, angiosarcoma) and may also identify small vessels. In malignancy, EGE typically demonstrates dark areas with surrounding enhancement from necrotic tissue, while LGE can show enhancement due to expanded interstitial space such as in fibrosis (Figure 5.5). Such enhancement is absent in cystic lesions and most benign tumours, with exceptions being haemangiomas, myxomas and fibromas (Figure 5.6).