CARDIAC MALPOSITIONS INCLUDING HETEROTAXY SYNDROMES
Introduction
Dextrocardia and other cardiac malpositions are usually associated with complex congenital heart defects (CHDs). Furthermore, most physicians are flabbergasted when it comes to evaluation of a baby with cardiac malposition. In this chapter, an orderly, methodical, and systematic approach is presented, hoping to make the evaluating physician more comfortable in approaching an infant with cardiac malposition.
Cardiac Malposition
Definitions – Terminology
Normally, the heart is in the left side of the chest (Figure 36.1) and is described as levocardia. If the heart is in the right side of the chest (Figure 36.2), it is called dextrocardia; or it may be in the middle of the chest (Figure 36.3) and is named mesocardia.1 Apicality of the heart cannot always be determined with certainty and is not necessary for the diagnostic approach, which will be described in this chapter.
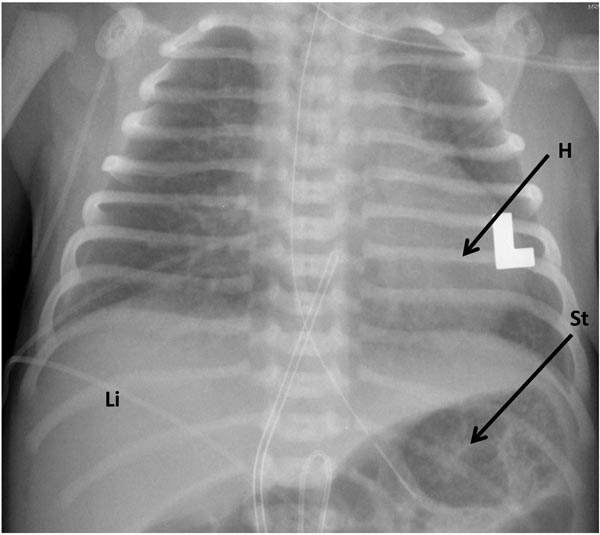
Figure 36.1. Normal position of the heart in the left side of the chest, also described as levocardia. The heart (H) is shown on the left side of the chest with the liver (Li) on the right and the stomach air bubble (St) in left side of the abdomen.
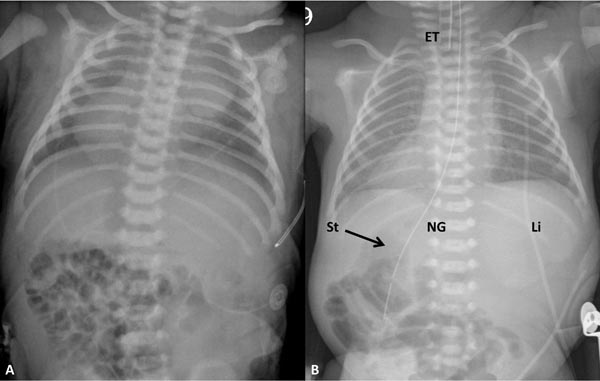
Figure 36.2. Chest x-rays of 2 neonates with dextrocardia. A: The liver is seen across the abdomen without air in the stomach, making it difficult to ascertain situs. B: The air in the stomach (St) is faintly seen on the right and the liver (Li) on the left side of the abdomen; these findings suggest situs inversus. In addition, the position of the stomach on the right is confirmed by the position of the nasogastric (NG) tube. ET, endotracheal tube.
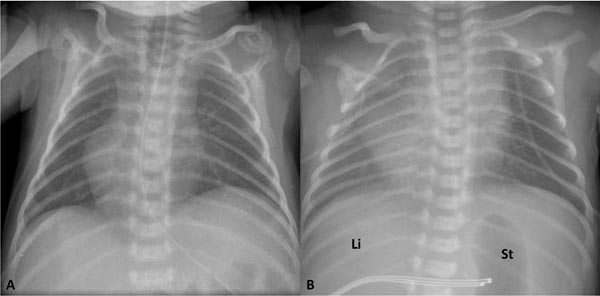
Figure 36.3. Chest x-rays of 2 neonates with mesocardia. A: The liver is seen across the abdomen without air in the stomach, making it difficult to ascertain situs. B: The air in the stomach (St) is faintly seen on the left and the liver (Li) on the right side of the abdomen; these findings suggest situs solitus.
The heart may be pushed (Figure 36.4 and 36.5) or pulled (Figure 36.6) to the right, in which case it is described as dextroposition.
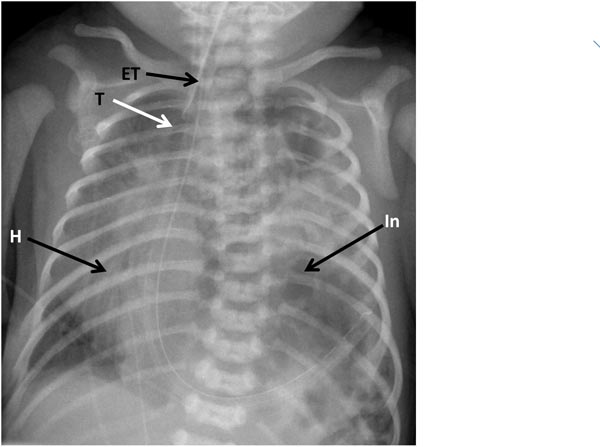
Figure 36.4. Chest x-ray of a neonate with dextroposition of the heart (H) due to diaphragmatic hernia on the left. The intestines (In) and other abdominal contents are in the left chest pushing the heart into the right chest. Note displacement of the trachea to the right. ET, endotracheal tube.
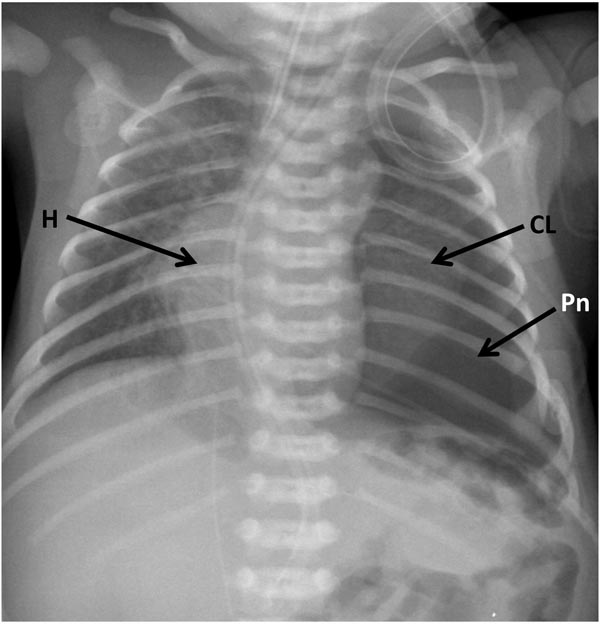
Figure 36.5. Chest x-ray of a neonate with dextroposition of the heart (H) due to pneumothorax (Pn) in the left chest pushing the heart into the right chest. Collapsed lung (CL) is shown.
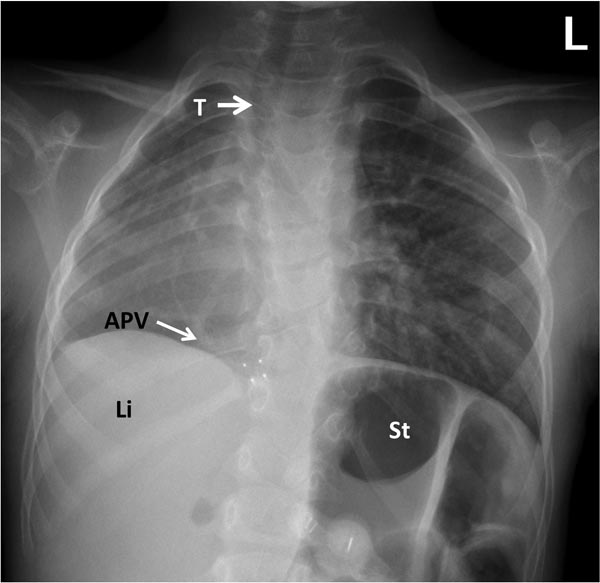
Figure 36.6. Chest x-ray of an infant with dextroposition of the heart due to Scimitar syndrome. The heart is pulled to the right because of hypoplasia of the right lung. Anomalous pulmonary vein is shown (arrow – APV); the name of the syndrome is derived from this vessel because of its shape (Scimitar). Also note the displacement of the trachea (T) to the right. Li, liver; St, stomach.
Definition of other terms used in this chapter is as follows:
- Situs solitus: Normal position of the viscera with the liver on the right side and the stomach on the left (see Figure 36.1).
- Situs inversus: Left-to-right reversal of the viscera with the stomach on the right and liver on the left (see Figures 36.2B and 36.7).
- Situs inversus totalis: Dextrocardia with situs inversus (see Figures 36.2B and 36.7).
- Isolated dextrocardia: Dextrocardia with situs solitus (Figure 36.8).
- Isolated levocardia: Levocardia with situs inversus (Figure 36.9).
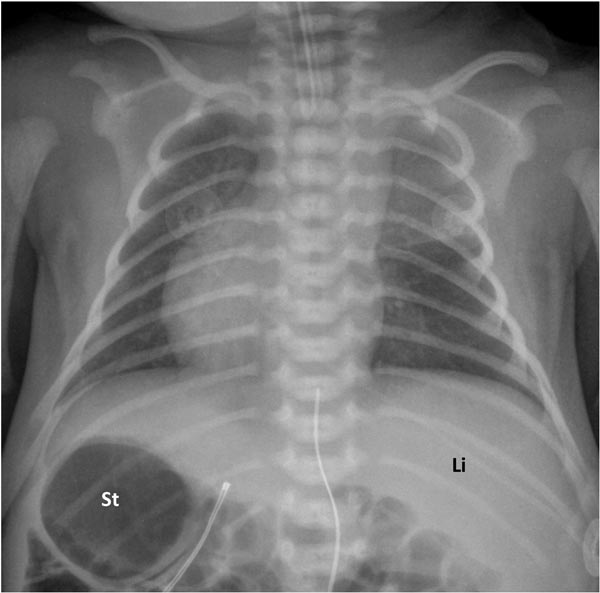
Figure 36.7. Chest x-ray of a neonate with dextrocardia and situs inversus, that is, situs inversus totalis. Li, liver; St, stomach.
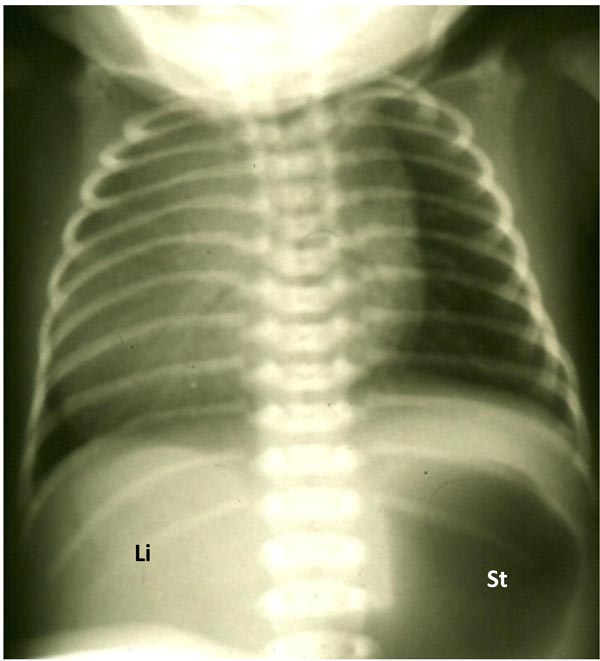
Figure 36.8. Chest x-ray of a neonate with isolated dextrocardia; that is, dextrocardia with situs solitus with the liver (Li) on the right and the stomach (St) on the left.
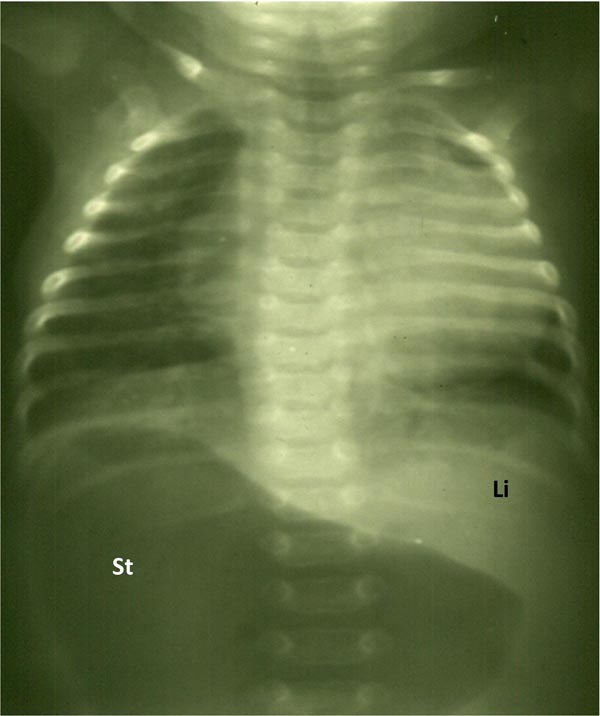
Figure 36.9. Chest x-ray of a neonate with isolated levocardia; that is, levocardia with situs inversus with the stomach (St) on the right and the liver (Li) on the left. Markedly dilated St is likely related to intestinal obstruction secondary to malrotation.
Dextroposition
Since the babies with dexroposition do not have a higher incidence of heart disease than normal babies, and because it is important to address the condition causing shift of the cardiac position, it is best to identify dextroposition first. The heart may be pushed to the right by thoracic cage abnormality, empyema, pneumothorax, lobar emphysema or diaphragmatic hernia on the left side or pulled to the right by collapse or hypoplasia of the right lung, including scimitar syndrome. Some of these are shown in Figures 36.4, 36.5 and 36.6. A careful review of the chest x-ray may indentify the abnormality causing dextroposition. In addition, deviation of the trachea to the right (see Figures 36.4, 36.5 and 36.6) will help in the diagnosis.
Prevalence
As mentioned above, heart is usually normal in dextroposition. In dextrocardia the prevalence of CHD is higher; this varies with the associated visceroatrial situs. In situs inversus totalis, CHD is present in 3% to 10% of the babies while in isolated dextrocardia and isolated levocardia, CHD is present in almost 100% of the babies. This is in contradistinction to less than 1% CHD prevalence in normal population.2,3
Segmental Analysis
The cardiac malposition is best evaluated by systematic segmental analysis.1 The approach is same whether the baby has levocardia, dextrocardia or mesocardia. Once dextroposition is excluded and it is determined that the location of heart in the chest is intrinsic or primary (ie, inherent cardiac malposition), the following questions should be addressed: (1) What is the visceroatrial situs? (2) Ventricular relationship: Are there 2 ventricles or 1? If 2, where are the ventricles located in relation to each other? (3) What is the status of atrioventricular (AV) connections? (4) How are the great arteries related to each other and with ventricles? (5) What is the conotruncal relationship?
What is the visceroatrial situs? It may be situs solitus, situs inversus or situs ambiguous (symmetricus or indeterminatus). There are number of methods by which the situs may be determined.
P waves in ECG. Normally the cardiac impulse originates in the sinoatrial node, located at the superior vena cava (SVC)–right atrial (RA) junction and traverses inferiorly and to the left. The resultant atrial depolarization produces P waves in the ECG. The P-wave axis is +45° (Figure 36.10) with positive P waves in leads I and AVF (Figure 35.11). This is indicative of situs solitus. In situs inversus, the atria are inverted and the P-wave axis will be around +135° (see Figure 36.10) giving negative P wave in lead I and positive P wave in lead AVF (Figure 35.12). If the P-wave axis is −45° (Figure 36.13) giving positive P waves in lead I and negative P in lead AVF, the so-called coronary sinus (CS) rhythm, the P axis may not be of much help in situs localization. However, as reviewed latter, coronary sinus rhythm is frequently seen in persistent left SVC and infrahepatic interruption of inferior vena cava (IVC), which in turn are associated with asplenia/polysplenia syndromes.
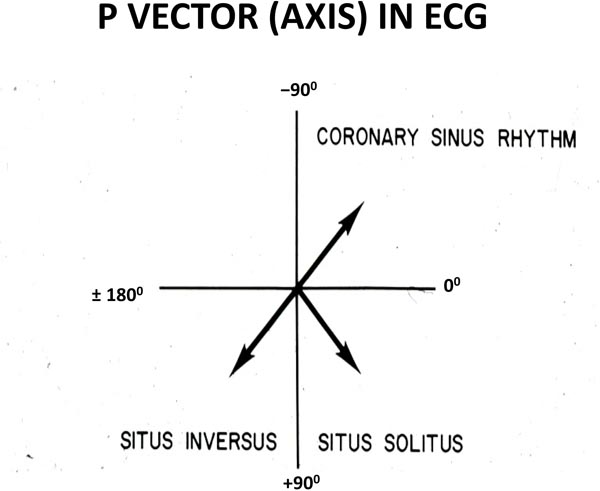
Figure 36.10. Usefulness of the P-wave axis (vector) in the frontal plane: P-wave axis between 0° and +90° suggests atrial situs solitus, P-wave axis between +90° and ±180° is indicative of situs inversus and P-wave axis between 0° and −90° is in favor of CS rhythm.
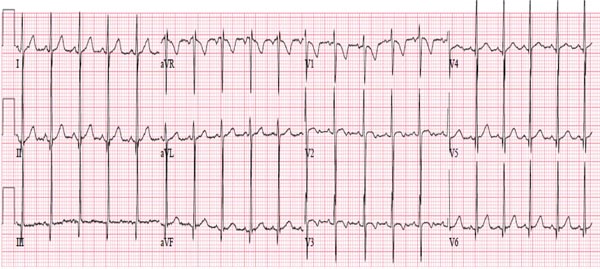
Figure 36.11. ECG of an infant demonstrating normal P-wave vector of +45° with positive P waves in both leads I and AVF; this indicative of situs solitus. Also note normal q waves in leads V5 and V6 and no q waves in right chest leads, suggesting normal interventricular relationship.
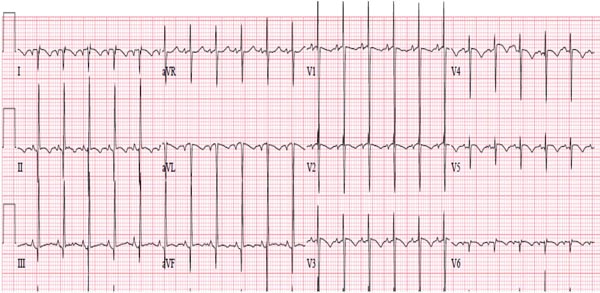
Figure 36.12. ECG of an infant demonstrating P-wave vector of +135° with negative P waves in lead I and positive P-wave AVF; this indicative of situs inversus. Note that there are no q waves in chest leads; this pattern is not useful in ventricular localization.
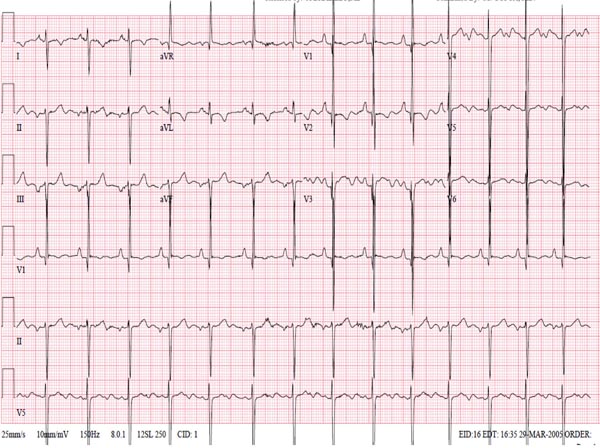
Figure 36.13. ECG of an infant demonstrating P-wave vector of −45° with positive P waves in lead I and negative P waves in lead AVF; this is indicative of CS rhythm, but is not helpful in situs localization. Also note q waves in right chest leads and no q waves in left chest leads; this is suggestive of ventricular inversion, although this can be seen in severe right ventricular hypertrophy.
Visceroatrial concordance. The general rule of visceroatrial concordance suggests that right-sided liver and left-sided stomach (see Figures 36.1, 36.3B and 36.8) are indicative that morphologic right atrium (RA) is on the right side and morphologic left atrium (LA) on the left side, that is, situs solitus. On the contrary, left-sided liver and right-sided stomach (see Figures 36.2, 36.7 and 36.9) are associated with morphologic RA on the left side and morphologic LA on the right side; that is, situs inversus. If the hepatic lobes are similar in size or midline liver (Figure 36.14) is present, irrespective of the position of the stomach, situs ambiguous may be present and asplenia/polysplenia syndrome are likely.4 The principle of visceroatrial concordance is more reliable than P-wave vector in ECG in correctly identifying atrial situs.
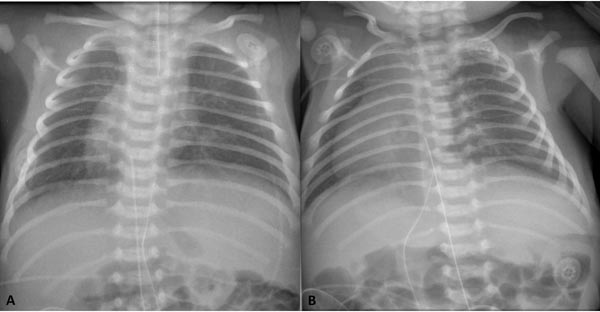
Figure 36.14. Chest x-rays of 2 neonates with dextrocardia with midline liver. These infants were later shown to have asplenia syndrome.
Tracheobronchial tree pattern. In normal babies with situs solitus, the right bronchus (RB) is short and wide and descends rather steeply while the left bronchus (LB) is long and narrow and descends more horizontally (Figures 36.15 and 36.16). In situs inversus, the tracheobronchial tree pattern is reversed (see Figures 36.15 and 36.17). This method appears to be more accurate than the 2 preceding methods.5,6 If both bronchi appear as morphologic right bronchi (see Figure 36.15), asplenia syndrome is likely while morphologic left bronchi on both sides (see Figure 36.14) are suggestive of polysplenia syndrome.1,4–6 Exception to these rules do occur but rare.1,4
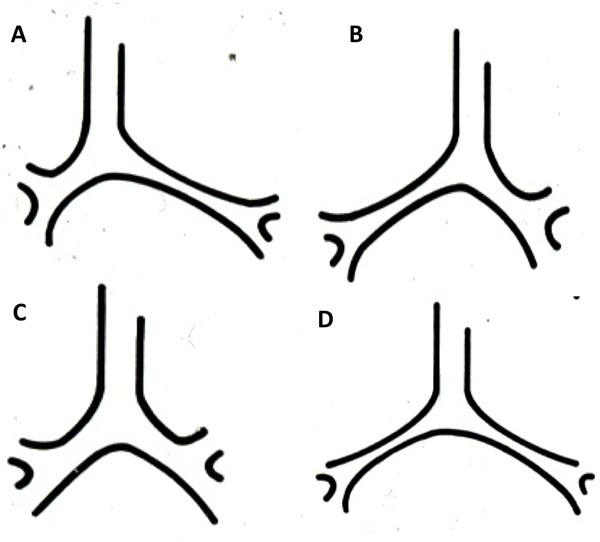
Figure 36.15. Diagrammatic portrayal of bronchial anatomy. A: In situs solitus, the RB is short and wide and descends rather steeply while the LB is long and narrow and descends more horizontally. B: In situs inversus, the tracheobronchial tree pattern is reversed with the morphologic RB on the left and the morphologic LB on the right. C: In asplenia syndrome, both bronchi appear as morphologic right bronchi. D: In polysplenia syndrome, both bronchi appear as morphologic left bronchi.
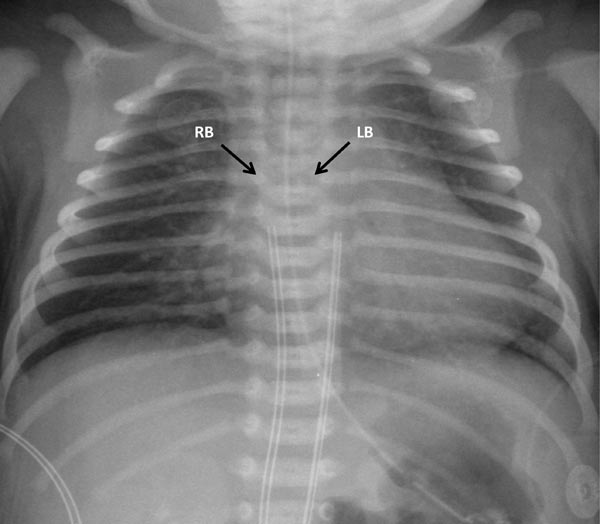
Figure 36.16. Chest x-ray of a neonate with situs solitus; the RB is short and wide and descends rather steeply, while the LB is long and narrow and descends more horizontally.
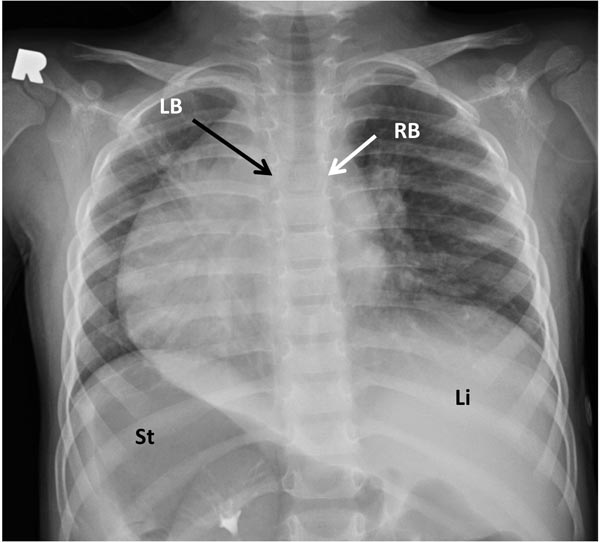
Figure 36.17. Chest x-ray of an infant with dextrocardia with the morphologic RB on the left and the morphologic LB is on the right, indicating situs inversus. The viscera are also inverted with the liver (Li) on the left and the stomach (St) on the right.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


