Acute rheumatic carditis is a common sequela of acute rheumatic fever. When it progresses to chronic rheumatic heart disease, it is a leading cause of heart failure in children and young adults, a common cause of cardiovascular mortality, and a predominant indication for cardiac surgery in poor countries.1,2,3,4
Acute rheumatic fever affects millions of people worldwide, and there are probably millions more that are not diagnosed.5 The incidence in the United States is somewhat less than 1 in 100,000, compared to 19 per 100,000 worldwide, and over 50 per 100,000 in high-risk regions such as Northern India.6
The incidence of carditis in children with rheumatic fever is as high as 50% to 60%,7 but the overall incidence is reported as 35% to 40%.5,6 The most common manifestations are mitral insufficiency and pericarditis. Although myocardial inflammation with interstitial Aschoff nodules is frequent, true myocarditis with myocyte necrosis is rare.8 Progression to chronic mitral and aortic valve disease occurs by adulthood in up to 60% of patients, almost half of whom do not recall a specific history of acute rheumatic fever.6
Risk factors for acute rheumatic fever include poverty, overcrowding, malnutrition, and maternal educational level and employment, but there are no identifiable risks for the development of acute pancarditis associated with the disease.9,10
Clinical Findings
The first episode of acute rheumatic fever usually occurs in children and young adolescents aged 5 to 14 years old. Presentation in those younger than 2 years or older than 35 years of age is rare.6
The clinical diagnosis of acute rheumatic fever is based on modified Jones criteria. Cardiac involvement is determined by significant apical systolic and/or basal diastolic murmurs, presence of pericarditis or unexplained congestive heart failure, and echocardiography or magnetic resonance imaging findings.11,12,13 Carditis may be isolated, or associated with chorea or arthritis, or both.7 Pericarditis and congestive heart failure almost never occur in the absence of valvular involvement, suggesting that primary myocarditis is uncommon.13
Rheumatic carditis is either primary or recurrent; recurrences are rare if the initial bout of rheumatic fever did not involve the heart. Recurrences are clinically defined as acute pericarditis or abrupt change in cardiac findings and are often difficult to diagnose if there is significant valvular disease. The use of Jones criteria in the evaluation of recurrent rheumatic fever is debated.1 Despite antibiotic prophylaxis for secondary prevention, carditis frequently recurs especially when there is poor compliance. These recurrent episodes tend to mimic the initial attack and generally occur within the first 5 years.6
Clinically, acute rheumatic carditis results in sinus tachycardia, an extended PR interval on electrocardiogram and a pansystolic murmur. The most common functional lesion is mitral regurgitation due to acute valvulitis. Pericarditis may cause chest pain and pericardial friction in cases with effusion, but cardiac tamponade is rare.14,15 Fulminant valvulitis causing death is also rare.16 Subclinical valvulitis as seen on echocardiographic studies is not uncommon.11,12,17 The risk of developing chronic rheumatic heart disease has been shown to directly correlate with the severity of carditis during the initial attack (Table 147.1).6
Pathogenesis
Acute rheumatic fever occurs as a sequel to upper respiratory tract infection by group A β-hemolytic streptococcal infections. The time interval between infection and systemic symptoms is commonly 2 to 5 weeks. The true pathogenesis of the carditis in rheumatic fever is unknown, and likely involves an altered immune response consisting of antibody-mediated and cellular components against cardiac proteins that show cross-reaction with epitopes from the bacteria. The adherence proteins M, T, and R of the microorganism probably share antigenic and molecular mimicry with several cardiac proteins such as cardiac myosin, tropomyosin, keratin, laminin, and vimentin. Different patterns of T-cell antigen cross-recognition have been identified in the process.18 Another theory relates to the damage caused to the endothelial collagen matrix type IV collagen, which may explain the more systemic nature of the process in some individuals.19 Cross-reactive antibodies bind to the endothelium with associated inflammatory infiltrates that mediate the up-regulation of VCAM-1.20,21
Pathologic Findings
The cardiac involvement by acute rheumatic fever usually involves endocardium, myocardium, and pericardium to various degrees, with at least half the patients presenting with cardiac inflammation involving the valvular endocardium (Table 147.2).17,22
Historically, Aschoff nodules have been described as the hallmark of rheumatic fever. Several studies have shown a high percentage of this finding in surgical specimens and endomyocardial biopsies in the older literature. The incidence of Aschoff bodies in the left atrial appendage ranges from 20% to 80% when these specimens were routinely removed during mitral commissurotomy for stenosis.23,24 The presence of Aschoff nodules was also highly detected in autopsy studies from patients dying from acute rheumatic fever and can also be seen years after the initial illness, with no correlation with activity or severity of disease.23,24,25 In endomyocardial biopsies, the frequency of finding Aschoff nodules is lower than in open surgical specimens, probably due to sampling, but one study found them in 22% of cases with suspected carditis clinically.26 A more recent study observed Aschoff nodules in 21% of the myocardium of acute rheumatic fever patients undergoing valve replacement or repair procedures.27
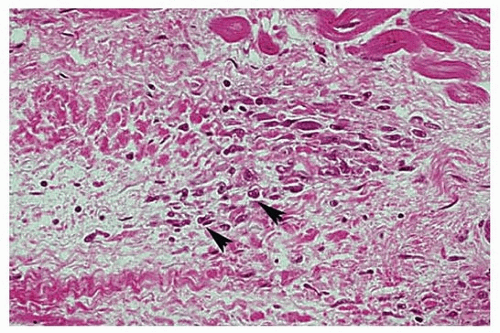
Histologically, Aschoff nodules are characterized by a histiocytic-rich lesion that resembles a granuloma and that is round or oval, usually in the endocardium or in the perivascular regions of the myocardium (Figs. 147.1 and 147.2). There is a central area of fibrinoid necrosis surrounded by histiocytes that show a basophilic cytoplasm and a vesicular nucleus. These histiocytes have been denominated by Anitschkow cells or Aschoff cells (Fig. 147.3).
Established myocardial necrosis is only seldom present in endomyocardial biopsies from patients with confirmed rheumatic fever,19,26 confirming clinical studies that only rarely show evidence of myocardial troponin elevations in the serum.8,13
In acute rheumatic fever, pericarditis is present in about one-fifth of the cases with confirmed histology, generally associated with underlying chronic inflammation. Pericarditis is usually fibrinous, with some cases showing the typical “bread and butter” appearance.28 There is an overlying fibrin layer and associated inflammatory infiltrates in the stroma with edema and the presence of Aschoff nodules, especially in a perivascular distribution. Chronic fibrinous pericarditis is a rare phenomenon after resolution of the acute disease.29
TABLE 147.1 Evolution of Rheumatic Heart Disease
Streptococcal Infection
Acute Rheumatic Fever (ARF)
Acute Rheumatic Carditis
Chronic Rheumatic Heart Disease
Incidence/frequency
Ubiquitous
<1-50/100,000 incidence; 0.3% of streptococcal pharyngitis
Unknown; aggressive treatment of carditis with anti-inflammatory agents does not significantly decrease risk
Initially severe carditis; recurrences
aMany adults with typical findings of postinflammatory mitral/aortic valve disease (40%-50%) have no documented history of acute rheumatic fever as a child; therefore, true incidence is unknown.
TABLE 147.2 Most Common Gross and Histologic Findings in Specimens of Acute Rheumatic Carditis.
Site of Lesions
Gross Findings
Microscopic Findings
Endocardium
Small friable vegetations on atrial surface of atrioventricular valves and ventricular surface of semilunar valves
Edema and granulation tissue
Valvular fibrosis and chordal fusion in chronic lesions
Edema and inflammatory infiltrates in the various layers
Underlying chronic inflammation with lymphocytes and plasma cells
Aschoff bodies
Myocardium
Most commonly no gross abnormalities
Globular enlargement if fatal cases
Edema and nonspecific inflammation
Debatable if there are true foci of myocardial necrosis
Aschoff bodies, if present, are usually in the perivascular regions of the interventricular septum and posterior wall of LV
Pericardium
Fibrinous pericarditis in about 1/5 of cases
Fibrous plaques may be present
Rarely the lesions persist with fibrous adhesions
Fibrin layer with underlying acute and chronic inflammatory infiltrates
Aschoff bodies more common in younger patients
Acute rheumatic fever may cause significant endocardial and consequently valvar inflammatory lesions, generally characterized by small 1- to 2-mm fibrinous vegetations seen on the atrial surface at sites of valve closure (Fig. 147.4). Histologically, they are associated with underlying chronic inflammatory infiltrates involving the valve leaflet, unlike marantic endocarditis. Aschoff bodies have been reported in the valvar tissue with variable prevalence.23,28 Examination of valves reveals that the mitral valve is most commonly affected, followed by the aortic, tricuspid, and, uncommonly, pulmonic valve. Valvular fibrosis occurs over time, when the disease progress to chronic rheumatic disease with regurgitation and/or stenosis clinically.
FIGURE 147.1 ▲ Aschoff nodule. There is an interstitial aggregate of macrophages and degenerating collagen. There are scattered Anitschkow cells (arrows).
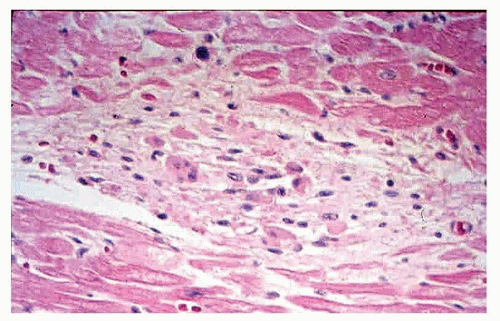
FIGURE 147.2 ▲ Aschoff nodule. There is vaguely granulomatous aggregate in the interstitium, with macrophages and lymphocytes.
Treatment and Prognosis
The treatment of acute rheumatic fever aims first and foremost to eradicate the streptococci to avoid repetitive exposure to the bacterial antigens. However, antimicrobial therapy does not affect the frequency or severity of rheumatic carditis, and there is little consensus about therapy to prevent cardiac sequelae.30 Treatment of the acute illness includes intravenous immunoglobulin, salicylates, and steroids.6,10 The surgical treatment of valvular lesions is only rarely used in the acute setting and reserved for chronic rheumatic valvular disease.
Most patients recover from an episode of acute rheumatic carditis without sequelae, but the outcome worsens if the episodes recur.4 Therefore, overall prognosis is mostly dependent on severity of carditis and recurrent episodes of rheumatic fever.22 In all, it is estimated that 60% of patients will at one time in their lives develop chronic heart valve disease.5,6
Only gold members can continue reading. Log In or Register to continue