(1)
Department of Neuroscience, University of Turin Ospedale Molinette, Turin, Italy
Abstract
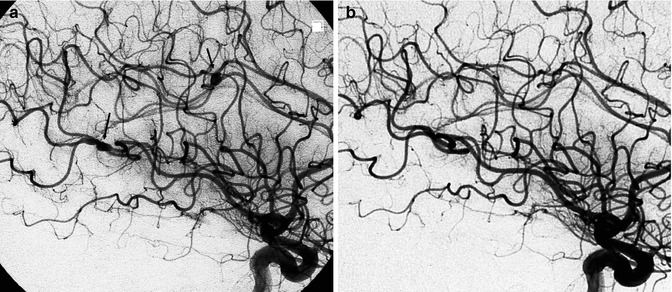
There are many cardiac diseases responsible for cerebral ischemia, which is frequently the result of emboli in patients with cardiac dysrhythmia, myocardial infarction, atrial septal aneurysm, cardiac valves diseases, prosthetic valves, endocarditis of various origins, and congenital heart diseases. Recently, paradoxical embolism through a patent foramen ovale has become a frequent explanation for embolism (Lechat et al. 1988). Cardiac abnormalities responsible for embolization have been identified in systemic lupus erythematosus and in primary antiphospholipid antibody syndrome. Another rare pathology is myxoma. This is a tumor that commonly originates in the left atrium in young to middle-aged patients. The emboli consist of myxomatous tissue that leads to parenchymal tumoral localizations and vascular changes, with occlusion and aneurysmal dilation (New et al. 1970) (Fig. 18.4).
There are many cardiac diseases responsible for cerebral ischemia, which is frequently the result of emboli in patients with cardiac dysrhythmia, myocardial infarction, atrial septal aneurysm, cardiac valves diseases, prosthetic valves, endocarditis of various origins, and congenital heart diseases. Recently, paradoxical embolism through a patent foramen ovale has become a frequent explanation for embolism (Lechat et al. 1988). Cardiac abnormalities responsible for embolization have been identified in systemic lupus erythematosus and in primary antiphospholipid antibody syndrome. Another rare pathology is myxoma. This is a tumor that commonly originates in the left atrium in young to middle-aged patients. The emboli consist of myxomatous tissue that leads to parenchymal tumoral localizations and vascular changes, with occlusion and aneurysmal dilation (New et al. 1970) (Fig. 18.4).
The commonest site of cardiac emboli is the anterior circulation, especially in the terminal internal carotid artery and in the middle cerebral artery territory. The posterior circulation is less involved, with a typical location being that of the top of the basilar artery. The incidence of cardioembolism is reported to be 15–20 % of all strokes (see also Chap. 15). It is most frequent in young patients (Barnett 1974; Barnett et al. 1980; Bogousslavsky et al. 1988a, b; Kittner et al. 1991; Broderick et al. 1992). As in other types of embolization, spontaneous rapid recanalization can occur, so angiography performed later appears normal.
In other cases occlusion is visible and a cardiogenic brain embolism can be clearly suspected when a specific cardiac pathology is present, more than one vascular territory is involved, or the stroke has occurred in patients younger than 45 years of age where atherosclerotic changes of the extra-intracranial arteries are less frequent than in the elderly. It should be remembered here that in this group of young patients, spontaneous dissection is also a frequent cause of stroke (see Chap. 16). In other cases it can be difficult to establish whether the stroke has a cardiogenic origin or it is due to atherosclerotic changes of the extra-intracranial arteries when both pathologies are present in the given patient (In addition to the Figs. 18.1, 18.2, 18.3, and 18.4, see Figs. 15.9, 15.10, 15.11, 15.21, 15.22, 15.23, 15.24).