Sickle cell disease is a chronic hemolytic anemia caused by abnormal hemoglobin that polymerizes and deforms red blood cells into the characteristic sickle shape. There is a single nucleotide mutation in the gene coding of the β-hemoglobin chain that is inherited in an autosomal recessive fashion. Sickle cell crises cause episodes of microvascular occlusion and premature red blood cell destruction, which lead to chronic severe hemolytic anemia and microscopic infarcts in the brain, lung, bone, kidney, liver, spleen, and retina.
The most common cardiac manifestation of sickle cell disease is high-output heart failure secondary to chronic anemia. Left ventricular mass is increased secondary to compensatory hypertrophy, which occurs in response to ventricular dilatation.1
Primary cardiac damage in sickle cell disease is theoretically possible through two mechanisms: direct iron toxicity due to myocyte iron overload and ischemic change secondary to microscopic thrombosis. Despite the frequent assertion that there is increased iron within the myocytes of patients with sickle cell disease,2 there is little if any evidence to support this view pathologically.
Clinically, iron overload in the heart, liver, and pancreas is assessed by magnetic resonance imaging. Myocardial iron overload as assessed by magnetic resonance imaging (T2) has been shown to occur in only a small percentage of chronically transfused sickle cell disease patients.1 One study of 23 patients showed no myocardial iron accumulation.3 Those patients at risk have exceptionally poor chelation control of total body iron stores and very high levels of hemoglobin S, reticulocytes, and serum transferrin.4 There have been no reports of invasive procedures (i.e., endomyocardial biopsy) documenting the presence of myocardial iron related to iron overload in sickle cell disease.
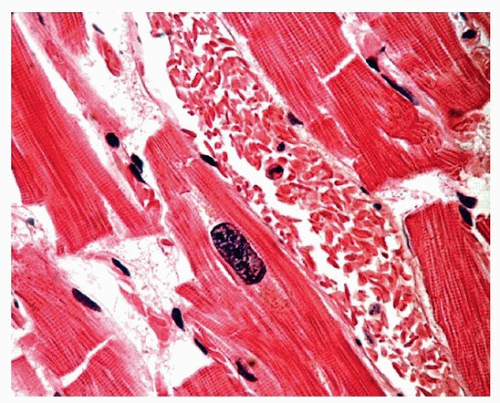
FIGURE 145.1 ▲ Drepanocytosis (sickling of erythrocytes) in myocardial vessel. This is a constant finding in patients dying with sickle cell disease but is also seen in 95% of patients dying with sickle cell trait. See reference.7
Approximately 10% of patients with sickle cell crisis have evidence of enzyme leak with elevated troponins, and chest pain may occur.5 Myocardial perfusion defects have been described by single photon emission computed tomography.6 By cardiac magnetic resonance imaging using late gadolinium enhancement, only 13% of sickle cell patients had evidence of myocardial fibrosis.1
There is a paucity of autopsy studies documenting the pathologic features of ischemic lesions in sickle cell disease (Figs. 145.1 and 145.2).8 Microvascular occlusions resulting in ischemic scars, sometimes termed “sludge infarcts,”9 have been related to sickle cell “vasculopathy.”10 One autopsy study demonstrated acute infarcts in 3 and healed infarcts in 4 of 72 patients with sickle cell disease and documented intramural coronary thrombi.11 A different autopsy study of over 50 patients did not demonstrate evidence of intramural coronary occlusion or infarcts, but showed secondary changes related to atherosclerosis, pulmonary hypertension, and systemic hypertension. The term “cardiomyopathy of sickle cell disease” was therefore not recommended.12
Sickle cell disease often causes right ventricular hypertrophy and dilatation secondary to pulmonary vascular occlusive disease and pulmonary hypertension.
Pathophysiology of Cardiac Iron Overload
As serum transferrin becomes saturated, iron that is not bound to transferrin is released into the circulation, which can enter hepatic, pancreatic, and other organ tissue including the myocardium. Ferrous iron enters cardiac myocytes through L-type calcium channels where it is bound to ferritin. As the capacity of ferritin to store iron is exceeded, it is released in the form of hemosiderin and free iron into the cytoplasm. Cardiac damage is the result of oxidation and formation of free radical hydroxyl ions that cause lipid peroxidation and increased membrane permeability.13
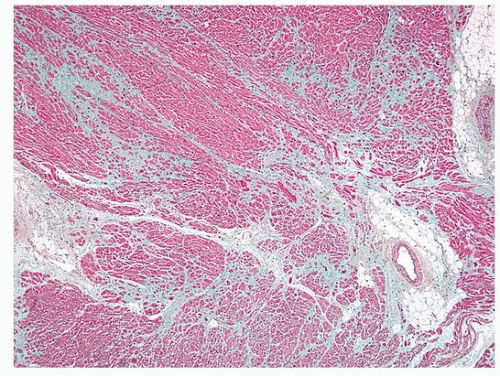
FIGURE 145.2 ▲ Sickle cell disease, patchy scarring. Sickle cell disease may cause patchy scarring in the myocardium, presumably caused by areas of healed ischemia from microvascular disease.
TABLE 145.1 Conditions Associated with Tissue Iron Overload, and Cardiac Involvement
Cardiac iron overload is caused by a variety of conditions including genetic (hemochromatosis) and acquired (see Table 145.1). Friedreich ataxia is considered in more detail in Chapter 160.
Transfusions are a major contributor to cardiac iron overload in cases of hemolytic anemias and hemoglobinopathies, with a minor contribution by hemolysis. Supplemental iron infusions may rarely result in iron overload involving the heart.16,18 Cardiac iron overload is characteristic of hemochromatosis and thalassemia and plays a minor role in other hemoglobinopathies, such as sickle cell disease. Iron overload may interact with other processes that contribute to heart failure, such as anthracycline toxicity or, more commonly, high-output failure related to anemia.13
Only gold members can continue reading. Log In or Register to continue