Chapter 9
Cardiac CT Angiography
1. What are the contraindications for cardiac computed tomography (CT)?
2. What is the difference between prospective triggering and retrospective gating?
Prospective triggering is an axial (step-and-shoot) image technique that acquires images of the heart in a predetermined phase of the cardiac cycle, for example 60% to 80% of the R-R interval. During the remainder of the cardiac cycle, the CT tube current is turned off. This is in contrast to retrospective gating, which is a spiral acquisition where the CT tube current remains on during the entire R-R interval. To reduce radiation, the tube current may be decreased during systole (electrocardiography [ECG] tube current modulation). However, there is a significant reduction in radiation dose when using prospective triggering (Fig. 9-1).
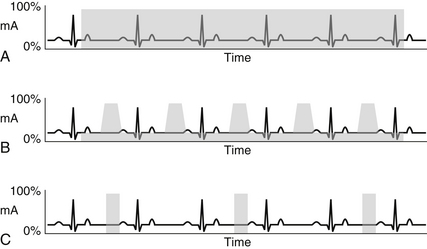
Figure 9-1 Schematic drawings of retrospective gating (A, B) and prospective triggering (C) techniques. Retrospective gating without tube current modulation (A) uses full tube current throughout the duration of the cardiac cycle. With tube current modulation applied (B), the full current is only delivered during a specified portion of the R-R interval (usually late diastole). In this case, the remainder of the cardiac cycle receives only 20% of the full tube current. Prospective triggering (C) only uses full tube current through a specified portion of the R-R interval. Every other heartbeat is imaged in prospective triggering to allow time for table movement.
3. When might retrospective gating be used rather than prospective triggering?
Retrospective gating is needed when cardiac function measurements are needed. Because images are acquired throughout the cardiac cycle, volume measurements of the right and left ventricles can be obtained in end-systole and end-diastole, allowing the calculation of stroke volume, ejection fraction, and cardiac output. Retrospective gating is also helpful in patients with irregular heart rhythm to help ensure diagnostic images of the coronary arteries are acquired. In contrast to prospective triggering, retrospective gating allows the user to employ ECG editing to remove artifacts related to premature ventricular contractions or dropped beats.
4. What is the radiation dose of a standard cardiac CT examination?
The radiation dose of a standard cardiac CTA depends on a multitude of factors and can range from less than 1 mSv to as high as 30 mSv with older high dose techniques and scanners. The median dose in an older registry study showed the cardiac CT dose to be just less than 10 mSv; however, since that time, there has been development of several new scanners and associated hardware, as well as new dose reduction strategies. At several hospitals (such as Massachusetts General Hospital), the median reported dose ranges from 3 to 5 mSv. To put things in perspective, the average dose from a nuclear perfusion stress test is 6 to 25 mSv (or as high as 40 mSv or more in thallium stress/rest tests), and the average dose from a simple diagnostic coronary angiogram is 5 to 7 mSv. Factors affecting the radiation dose of a cardiac CT include the type of scanner (single-source versus dual-source), the number of detectors (z-axis coverage), the body habitus of the patient, the selection of kilovolt peak (kVp) and milliampere seconds (mAs), and the scan mode (prospective triggering versus retrospective gating with or with or without tube current modulation, high pitch [FLASH] acquisitions). General measures to reduce the radiation dose to the patient should be used whenever possible, according to the “as low as reasonably achievable” (ALARA) principle. Tube modulation routinely should be applied if retrospective gating is selected, unless a specific reason prohibits its use (Fig. 9-2).
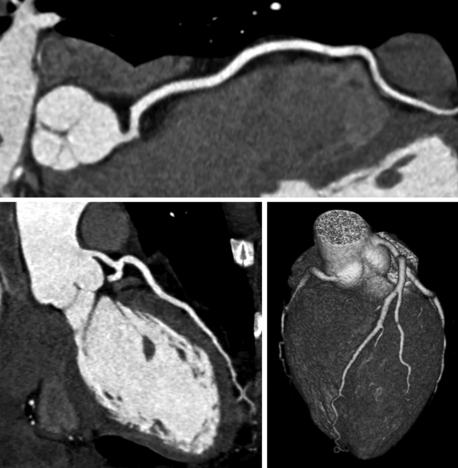
Figure 9-2 Curved multiplanar reconstructions of the right coronary artery (top) and left anterior descending coronary artery (bottom left) and volume-rendered three-dimensional reconstruction (bottom right) show absence of coronary plaque or stenosis. A negative computed tomography scan with good image quality has a very high negative predictive value and may spare the patient a diagnostic invasive angiogram. This study was done with a total radiation dose of 2.4 mSv.
5. What is blooming and what techniques can be done to reduce it?
Blooming is an artifact created when material with very high attenuation is being imaged. The borders of a high-attenuation material will “bleed” into adjacent structures. In the case of coronary CTA, blooming from calcified plaque can lead to overestimation of the degree of coronary stenosis. For this reason, a very high calcium score (generally greater than 1000) may yield nonevaluable coronary artery segments. Using a higher current (mA) and/or tube potential (kVp) can reduce blooming artifact. Using a sharp reconstruction kernel and thin slices can help in postprocessing and interpretation (Fig. 9-3).
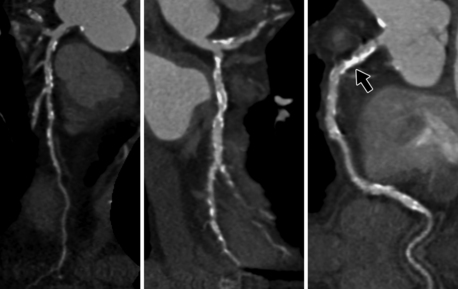
Figure 9-3 Curved multiplanar reconstructions of the left anterior descending coronary artery (left), left circumflex coronary artery (middle), and right coronary artery (right) demonstrate substantial calcification with blooming artifact. Evaluation of the degree of stenosis is limited in areas of extensive calcification, for example in the proximal right coronary artery (arrow). This patient had a calcium score of 867.
6. Are β-blockers necessary for coronary CTA?
7. A 66-year-old man with diabetes and smoking history comes to your clinic because he wants to check his calcium score. He states he read in a magazine that it is a good screening test for coronary artery disease (CAD). What is your response?
A calcium score is a specialized cardiac CT without contrast that is processed with software to quantify the amount of coronary calcium. This number, the Agatston score, is used as a surrogate for the total amount of coronary plaque and is correlated with patients of the same age and gender. It is most useful in patients with unclear or intermediate CAD risk, to guide decision-making. Whether this patient in question has a high or low calcium score, he is already considered high risk (ATP III/Framingham) and should be treated accordingly.
8. What is the value of a negative calcium score in a patient with low risk to intermediate risk?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


