Identify an intracardiac or extracardiac mass.
Demonstrate the extent and invasiveness of the mass (staging of tumor).
Distinguish between benign and malignant tumor, if possible.
Distinguish between primary and secondary tumor.
Distinguish between tumor and thrombus.
Differentiation of cardiac masses from normal anatomic variants
chronic obstructive pulmonary disease. Transesophageal echocardiography overcomes this problem but adds invasiveness. The soft tissue contrast achieved with echocardiography remains limited in comparison with that obtained with MRI and CT. Usually, pericardial involvement and infiltration of the myocardium can be better visualized with MRI and CT.
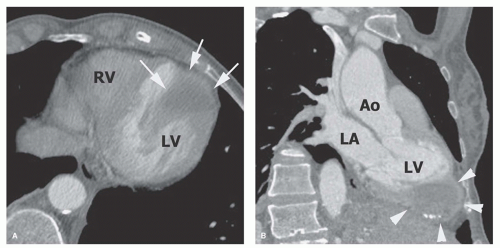 Figure 13.1. (A) Contrast-enhanced CT in the axial plane shows a low-density left ventricular mass involving the apex (arrows). (B) Coronal reconstruction from the CT better demonstrates the relationship of the mass (arrowheads) with the left ventricular apex. Note the peripheral rim of high density with some calcifications surrounding the lower-density central mass (fibroma). LV, left ventricle; LA, left atrium; RV, right ventricle; Ao, aorta. |
on T1-weighted images and moderate signal intensity on T2-weighted images. Cystic lesions (filled with simple fluid) have low signal intensity on T1-weighted images and high signal intensity on T2-weighted images (Fig. 13.5). The administration of Gd-DTPA (gadolinium diethylenetriamine pentaacetic acid) usually improves the contrast between tumor tissue and myocardium on T1-weighted images and may facilitate tissue characterization. Hyperenhancement of tumor tissue with MR contrast agents indicates either an enlarged extracellular space of tumor tissue in comparison
with normal myocardium (Fig. 13.6) or a high degree of vascularization of the mass. Application of a fat saturation sequence, which vitiates the bright signal of fat, is effective for the tissue characterization of lipomas (Fig. 13.7).
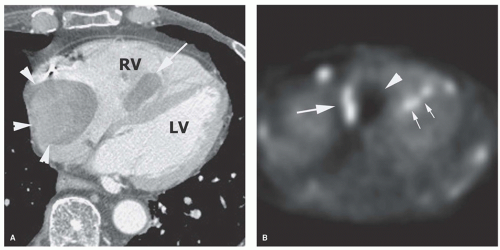 Figure 13.2. A: Axial contrast-enhanced CT image shows a right atrial mass (arrowheads) with a wide point of attachment to the wall. Note a second mass (arrow) within the right ventricle (RV). B: PET scan in the axial plane shows avid uptake of FDG in part of the atrial mass (large arrow) and in the ventricular mass (small arrows) in patient with metastatic thyroid cancer. Note that part of the atrial mass (arrowhead) has no uptake due to tumor necrosis. LV, left ventricle. |
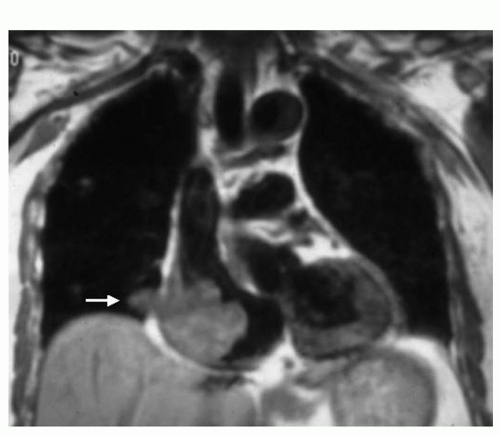 Figure 13.3. Angiosarcoma. ECG-gated spin-echo image in the coronal plane shows a large tumor in the right atrium extending through the atrial wall (arrow). The wide field of view of the coronal plane demonstrates the extent of this angiosarcoma. |
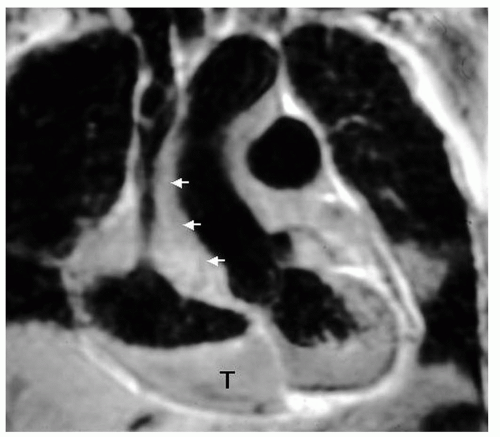 Figure 13.4. Angiosarcoma. ECG-gated spin-echo image in the coronal plane demonstrates a tumor (T) infiltrating through the right atrial cavity and extending around the superior vena cava (arrows). |
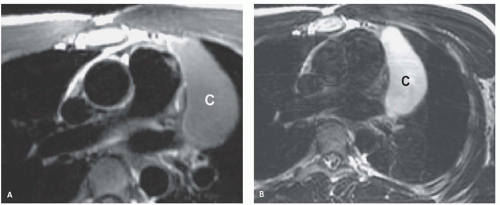 Figure 13.5. Pericardial cyst. ECG-gated spin-echo T1-weighted (A) and T2-weighted (B) images of a pericardial cyst (C). The simple fluid in the cyst has typical low signal on T1-weighted and homogeneous high signal on T2-weighted images. |
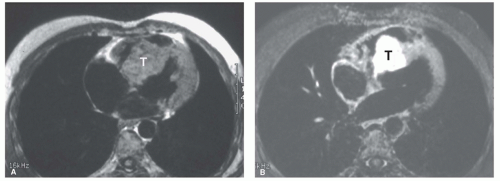 Figure 13.6. Angiosarcoma. ECG-gated spin-echo T1-weighted images before (A) and after (B) gadolinium chelate administration demonstrates hyperenhancement of the tumor (T) compared with the septal myocardium. The postcontrast image uses fat saturation. |
locally, they may lead to significant morbidity and mortality by causing arrhythmias, valvular obstruction, or embolism. An intramyocardial location can interfere with normal conduction pathways and produce arrhythmias, obstruct coronary blood flow, or diminish compliance or contractility through replacement of myocardium. Both benign and malignant tumors have characteristic sites of origin (Table 13.2).
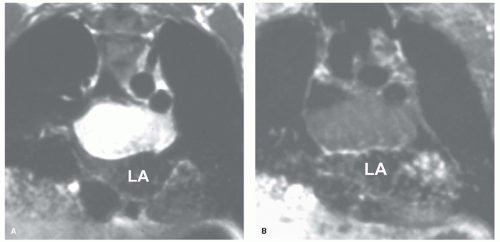 Figure 13.7. Lipoma. ECG-gated spin-echo images in coronal plane, before (A) and after (B) fat saturation, of a mass situated above the left atrium (LA). Signal of the mass is suppressed with fat saturation. |
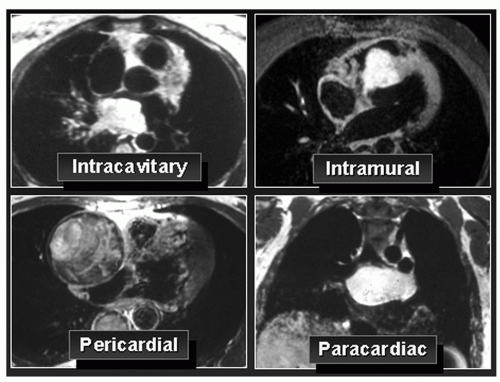 Figure 13.8. Location of masses on tomographic imaging. |
TABLE 13.1 Primary Benign Cardiac Tumors | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
TABLE 13.2 Typical Sites of Origin of Cardiac Tumors | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
atrioventricular valve (Fig. 13.10) or into the corresponding ventricle during diastole. Rarely, myxoma can have a wide point of attachment to ventricular endocardium (Figs. 13.11 and 13.12).
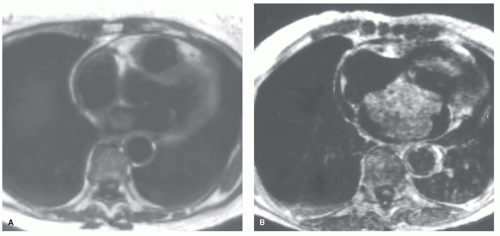 Figure 13.9. Myxomas. ECG-gated spin-echo images display two left atrial myxomas with a narrow point of attachment (pedicle; A) and a wide point of attachment (B) to the left side of the atrial septum. |
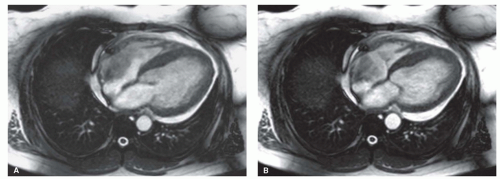 Figure 13.10. Myxoma. Cine MR images (balanced steady-state free precession) in the axial plane display a right atrial myxoma in diastole (A) and systole (B). The motion of the tumor is evident with movement into the tricuspid valve during diastole. |
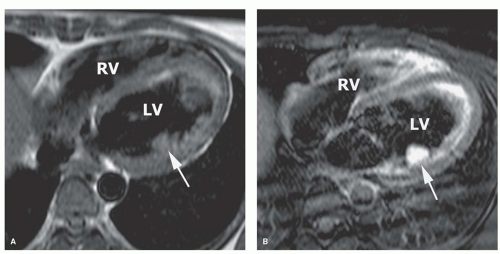 Figure 13.11. Left ventricular myxoma. T1-weighted axial spin-echo images before (A) and after (B) the administration of gadolinium chelate show a tumor (arrow) with a wide point of attachment to the left ventricular (LV) endocardium. Tumor markedly enhances after contrast media. Fat saturation was used after gadolinium. RV, right ventricle. |
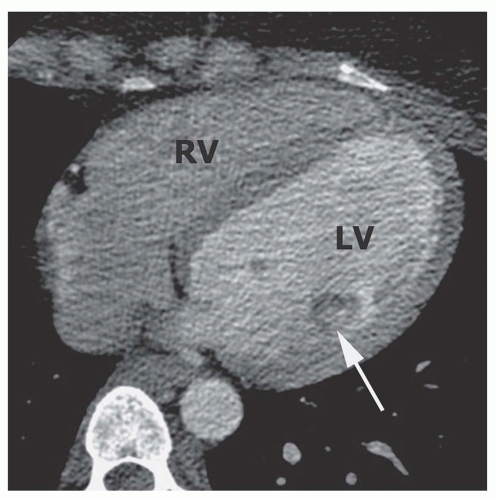 Figure 13.12. Contrast-enhanced CT in the axial plane shows the left ventricular myxoma (arrow) with some enhancement of the central part of the tumor. LV, left ventricle; RV, right ventricle. |
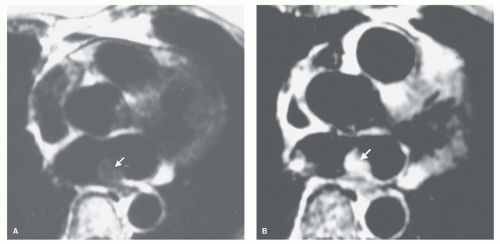 Figure 13.13. Myxoma. ECG-gated spin-echo images of a myxoma before (A) and after (B) gadolinium chelate administration. Tumor (arrows) increases substantially in signal intensity. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


