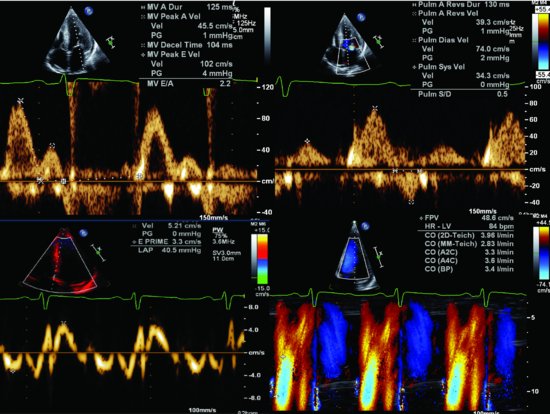
Figure 84.2 Doppler recordings of mitral valvular inflow, pulmonary vein inflow, pulse tissue Doppler, and the color M-mode indicated the pseudo normal pattern of diastolic dysfunction in case 1.
The aortic valve was trileaflet and structurally normal. The tricuspid and pulmonic valves were normal in structure and function. Trace tricuspid regurgitation was detected. The tricuspid regurgitant velocity was 2.52 m/sec; the estimated pulmonary artery systolic pressure was normal at 30.4 mmHg. A small pericardial effusion was present.
Case 2: Echocardiogram showed a severe concentric LV hypertrophy with restrictive diastolic dysfunction (Figure 84.3 b,c and Videoclip 84.1). Assessment of long-axis contraction using 2D strain imaging showed severe impairment in longitudinal strain, even the LV EF was within normal range (Figure 84.4). Cardiac catheterization showed normal coronary arteries. Cardiac biopsy showed amyloid deposits. Despite treatment with melphalan, prednisone, and adequate cardiac therapy, the patient died 8 months after the diagnosis of multiple myeloma due to intractable congestive heart failure.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


