Parameters
Conditions
Prospective data acquisition
At 80 % of R-R interval
Tube voltage
130 kVp
Tube current
(630 mA)
Slice thickness
(3 mm)
Acquisition time
(100 ms)
Contrast enhancement
None
Coronary artery calcium should be identified by analyzers with classifying branches.
Calcium area segmentation is semiautomatic using threshold technique, higher than 130 Hounsfield units (HU) and larger than single pixel.
The density of calcium area is stratified as “density factor” based on peak HU in two-dimensional ROI.
Density factors | Hounsfield units |
|---|---|
1 | 130–199 |
2 | 200–299 |
3 | 300–399 |
4 | Over 400 |
Agatston score (AS) is a global sum of products by calcium areas, density factors, and slice thickness.
 x, serial number of ROIs; A, area of ROIs; D, density factor; SL, slice thickness
x, serial number of ROIs; A, area of ROIs; D, density factor; SL, slice thickness
4.2.2 Volume Score [4]
The volume score (VS) was invented to overcome drawbacks of AS such as nonlinear measurement of HU (density factors) and complexity of measurement.
Scanning protocol and threshold value for segmentation are same as AS.
The VS is acquired as a global sum of ROI volumes.
The reproducibility of examination is higher by VS than by AS.
However, AS has greater reference standard criteria.
4.2.3 Mass Score [5]
Instead of adopting indirect parameters, the mass score (MS) was designed for more direct assessment of calcium mass.
Scanning field includes calcium hydroxyapatite [Ca10(PO4)6(OH)2, CaHA] phantoms as reference standard materials.
Initially, the HUs of CaHA phantoms are measured in corresponding images. Based on real calcium density in the phantoms, density-HU plotting with a linear fitting equation is possible.
![$$ HU=a\cdot \left[ CaHA\right]+b $$](/wp-content/uploads/2016/07/A311690_1_En_4_Chapter_Equc.gif)
[CaHA], calcium densities in CaHA phantoms
Since the calcium mass is a product of calcium density and its volume, the MS can be acquired from the fitting equation and the volume of ROIs.
![$$ MS={\displaystyle \sum}_{x=1}^n\left[\left(\frac{H{U}_x-b}{a}\right)\cdot {A}_x\cdot SL\right] $$](/wp-content/uploads/2016/07/A311690_1_En_4_Chapter_Equd.gif)
The strength of MS is the consistency of measured values throughout different scanning environments.
The MS is the most accurate and reproducible technique for CAC quantification.
Drawbacks of the MS are the complexity of assessment and lack of reference standard criteria for clinical application.
4.2.4 Other Scores
4.2.4.1 CAC Progression Rate [6]
Based on the fact that CAC increasing speed is associated with the risk of CAD, CAC progression rate (R) is suggested.
R reflects a percentile interval change of VS.
![$$ R=100\cdot {e}^{\left\{\frac{\varDelta \left[ \ln (VS)\right]}{T}\right\}-1} $$](/wp-content/uploads/2016/07/A311690_1_En_4_Chapter_Eque.gif)
T, time interval between examinations
The R may be a useful marker for a subsequent monitoring of the coronary atherosclerotic burden in single subject.
Drawbacks are the complexity of assessment and lack of the reference standard criteria.
4.2.4.2 Calcium Coverage Score [7]
The calcium coverage score (CCS) is the percentage of coronary arteries affected by calcium.
In a multiethnic large-scale cohort study, the CCS predicted cardiovascular events better than AS and MS.
A drawback is insufficient clinical application results including reference standard criteria.
4.3 Clinical Significance of CAC
4.3.1 Cardiovascular Risk by Plaque Burden (Figs. 4.1, 4.2, 4.3, 4.4, and 4.5)
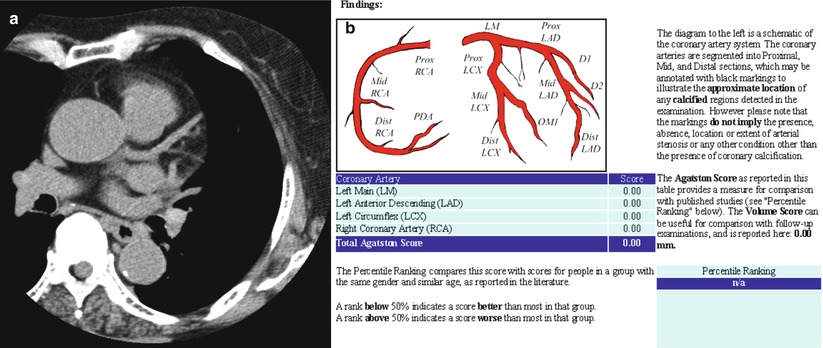
Fig. 4.1
A 72-year-old female. (a) Non-enhanced axial CT for calcium scoring shows no calcium in the coronary arteries. Small nodular calcification is noted in the descending aortic wall. (b) Total Agatston score is zero (From Hoff et al. [9])
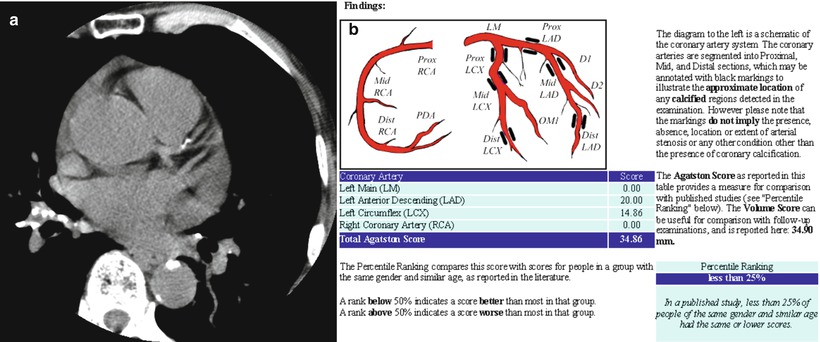
Fig. 4.2
A 77-year-old male. (a) Small calcific nodules are noted in the mid left anterior descending artery. Other calcific nodules are noted in the descending aortic wall and hilar lymph nodes. (b) Total Agatston score is 34.86, which means mild plaque burden. The subject is less than the 25th percentile in the same age and gender group (From Hoff et al. [9])
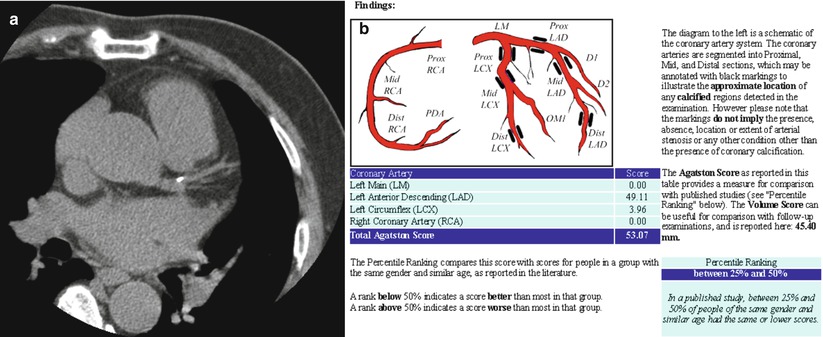
Fig. 4.3
A 69-year-old male. (a) Small nodular calcification is noted at the branching level of the left main coronary artery. (b) Total Agatston score is 53.07, which means mild plaque burden. Due to younger age than case 2, this subject is plotted between the 25th and 50th percentiles in the same age and gender group (From Hoff et al. [9])
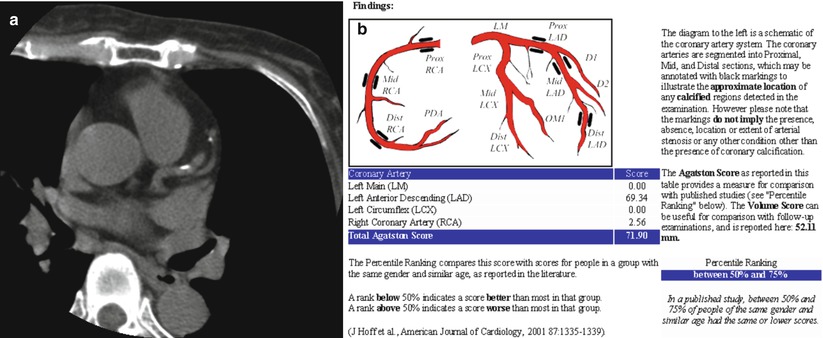
Fig. 4.4
A 71-year-old female. (a) Two calcific nodules are noted at the left anterior descending artery. (b) Total Agatston score is 71.90, which means mild plaque burden. Due to female gender, this subject is plotted between the 50th and 75th percentiles in the same age and gender group (From Hoff et al. [9])
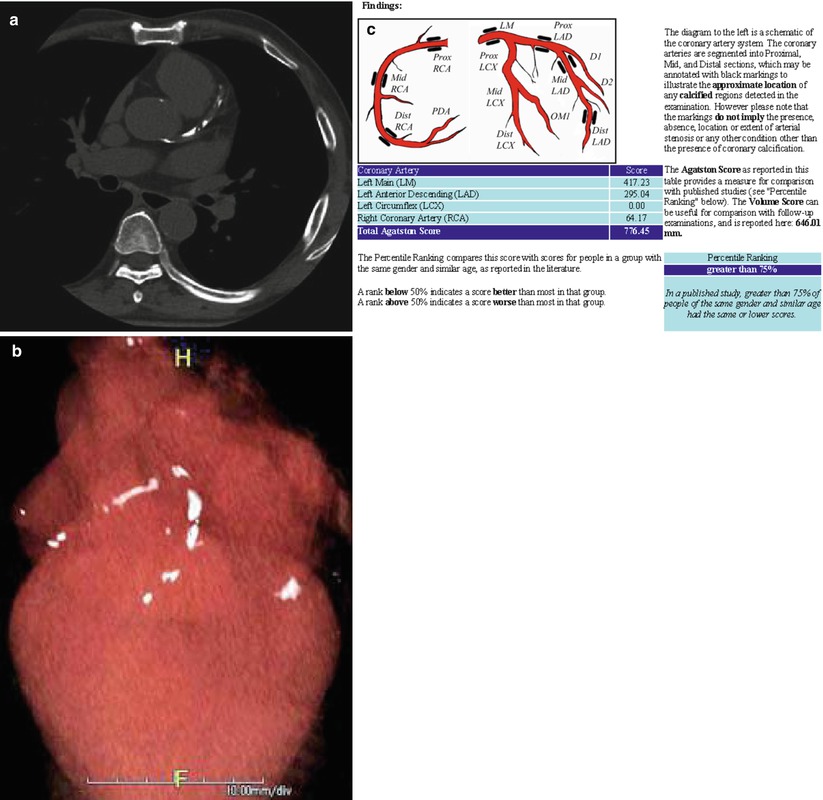
Fig. 4.5
A 61-year-old male with diabetes mellitus. (a) Diffuse calcification is noted from the orifice level of the left main coronary artery to the mid level of the left anterior descending artery. (b) Volume rendered 3-D image in 4-chamber orientation reveals heavy calcium in the left anterior descending and right coronary arteries. (c) Total Agatston score is 776.45, which means extensive plaque burden. This subject is stratified to higher than the 75th percentile in the same age and gender group. Stratification higher than the 75th percentile means high cardiovascular risk (From Hoff et al. [9])
An initial meta-analysis-based guideline for CAC Agatston score focused on plaque burden and its clinical interpretation (Table 4.1) [8].
Table 4.1
The interpretation guideline of Agatston score
Calcium score
Plaque burden
Clinical interpretation
0
None
Very low CVD risk
Less than 5 % chance of presence of CAD
A negative examination
1–10
Minimal
Significant CAD very unlikely
11–100
Mild
Likely mild or minimal coronary stenosis
101–400
Moderate
Moderate nonobstructive CAD highly likely
Over 400
Extensive
High likelihood of at least one significant coronary stenosis (>50 % diameter)
Nonlinear stratification of Agatston score matched with plaque burden and its clinical interpretation.
This guideline is simple to apply on routine practice.
However, diversity of CAC score by sex and age was not considered.
4.3.2 Cardiovascular Risk by Percentile Stratification (Figs. 4.1, 4.2, 4.3, 4.4, and 4.5)
Based on multicenter large cohort prospective research, Agatston score distributions by age strata and genders were suggested as an interpretation guideline (Table 4.2) [9].
Table 4.2
Distributions of Agatston score by age strata and genders
Percentile
Age (years)
<40
40–44
45–49
50–54
55–59
60–64
65–69
70–74
>74
Men
25th
0
0
0
1
4
13
32
64
166
50th
1
1
3
15
48
113
180
310
473
75th
3
9
36
103
215
410
566
892
1,071< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access
