(1)
Anatomy Department, University of Medicine and Pharmacy Carol Davila, Bucharest, Romania
Abstract
All boundaries of the heart are mediated by the fibrous pericardium. In Figs. 5.1, 5.2, 5.3, 5.4, 5.6, 5.7 and 5.22, different aspects of the rapports between the heart and pericardium are revealed.
All boundaries of the heart are mediated by the fibrous pericardium. In Figs. 5.1, 5.2, 5.3, 5.4, 5.6, 5.7 and 5.22, different aspects of the rapports between the heart and pericardium are revealed.
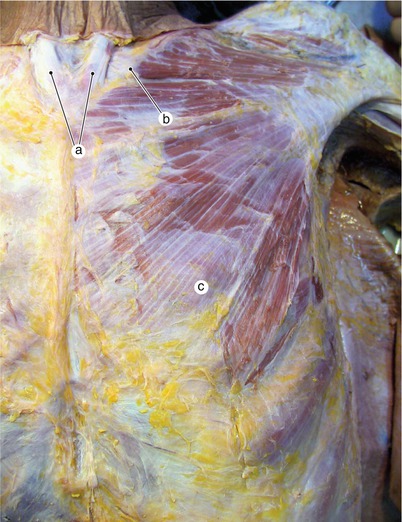
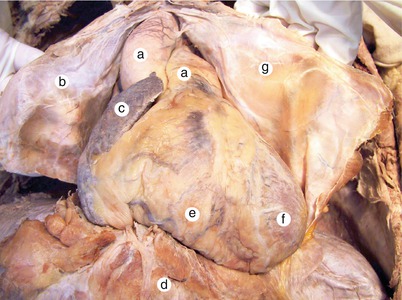
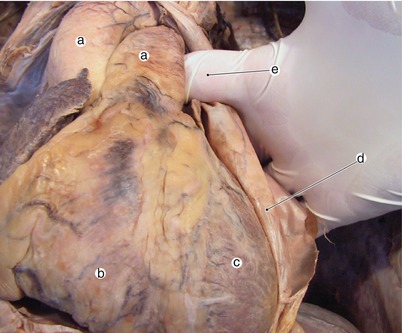
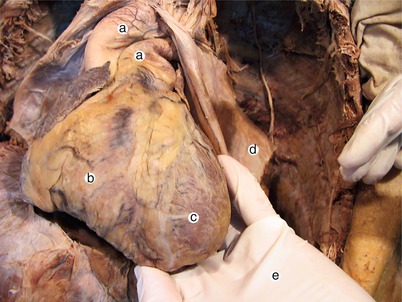

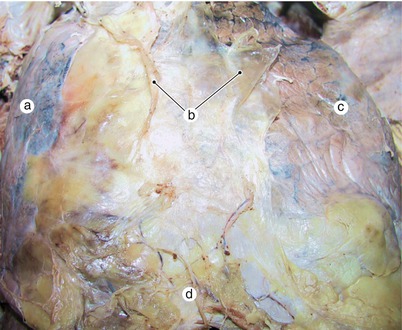
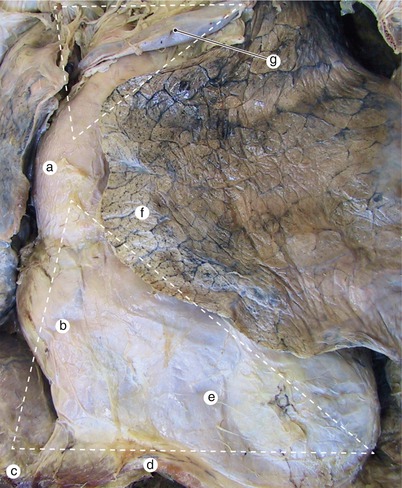
Fig. 5.1
Aspect of thoracic wall after removal of tegument. In the intercostal spaces, the thoracic wall is thin and can be easily perforated. a Insertion of the sternocleidomastoid muscles in the sternal notch, b clavicle, c pectoralis major muscle
Fig. 5.2
The pericardium has been sectioned and removed. Observe its location in relation to the greater vessels. a Arterial pedicle, b fibrous pericardium, c right auricle, d diaphragm, e right ventricle, f left ventricle, g fibrous pericardium
Fig. 5.3
Examiner’s finger is introduced behind the arterial pedicle, in the transverse pericardial sinus. a Arterial pedicle, b right ventricle, c left ventricle, d fibrous pericardium, e examiner’s finger into transverse pericardial sinus
Fig. 5.4
Examiner’s hand is introduced in the oblique pericardial sinus. a Arterial pedicle, b right ventricle, c left ventricle, d fibrous pericardium, e examiner’s finger into oblique pericardial sinus
Fig. 5.5
Line of fusion of pericardium to aorta. a Fibrous pericardium ascends on the arterial pedicle to reach the origin of the brachiocephalic trunk, b aorta, c arterial pedicle
Fig. 5.6
Aspect of thoracic organs after removal of the rib cage. Remark the difficulty in the indentification of the pulmonary and cardiac limits. a Right lung, b sectioned parietal pleurae, c left lung, d adipose tissue and retrosternal vascular network
Fig. 5.7
Pulmonary borders outline better the thymic trigon (superior) and cardiac trigon (inferior). a Ascending aorta, b right atrium, c inferior vena cava, d diaphragm, e heart in pericardial sac, f lingula, g left innominate vein
5.1 The Border with the Sternocostal Surface
This face is partially covered by the right and left costomediastinal recesses of the pleura. The anterior margins of the recesses are partially overlapped and they outline the thymic and cardiac triangles (Figs. 5.6, 5.7 and 5.8).
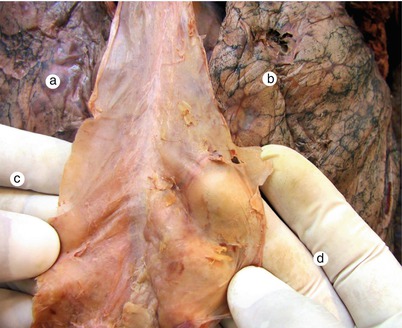
Fig. 5.8
Examiner’s fingers are introduced in the costomediastinal pleural recesses. The recesses are strengthened with loose connective tissue that, sometimes, can be hardly dissected. a Right lung, b left lung, c examiner’s fingers into right costomediastinal recess, d examiner’s fingers into left costomediastinal recess
Keep in mind!
Any instrumental access to the heart on its sternocostal surface must avoid puncturing the pleural recesses and opening of the pleural cavities.
5.1.1 Highlighting the Internal Thoracic Arteries
On the posterior face of the anterior thoracic wall, one centimeter from the sternum, the internal thoracic arteries descend (Fig. 5.9).

Fig. 5.9
Thoracic cage opened in the superior part. The internal thoracic vessels can be observed on both sides of the sternum. a Xiphoid process of sternum, b internal thoracic artery and veins, c body of sternum, d sternohyoid muscle, e transversus thoracic muscle, f internal intercostal muscle
Keep in mind!
To avoid perforating the left internal thoracic artery during cardiac punctures, the needle must be perpendicular to the thoracic wall and tangent on the sternum in the interspace between the fifth and sixth ribs.
Internal thoracic arteries are frequently utilized in coronary surgery. We consider that a minimum knowledge of the anatomy of these arteries is necessary.
The right internal thoracic artery is the first branch on the inferior face of the right subclavian artery. It descends in the thorax passing behind the brachiocephalic vein and intersects the right phrenic nerve under the clavicle. In its upper third it divides into the pericardiacophrenic and mediastinal branches. In the intercostal spaces it divides into the anterior intercostal and sternal branches (Figs. 5.10 and 5.11).
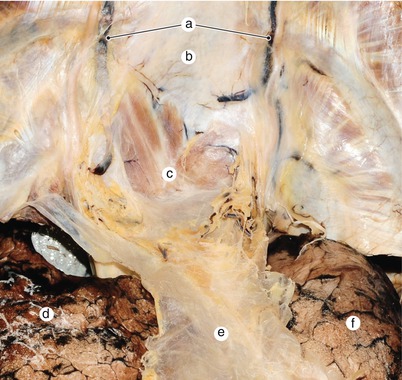
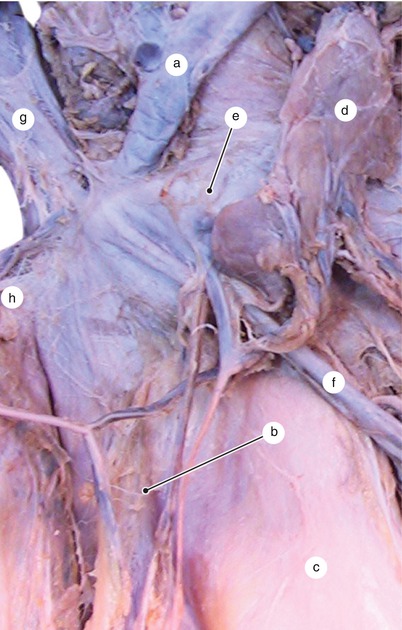
Fig. 5.10
Detail at the entrance of the internal thoracic arteries in the thorax. The ribcage is removed. The arteries descend between the pleurae and the sternocostal wall. a Internal thoracic arteries and veins, b sternum, c sternohyoid muscle, d right lung, e the costomediastinal pleural recesses, f left lung
Fig. 5.11
Thymus remainings are included between the venous plane and the sternocostal wall. a Inferior thyroid veins, b superior vena cava, c ascending aorta, d thymus remaining, e left innominate vein, f pericardiophrenic vein, g right internal jugular vein, h right subclavian vein
Both internal thoracic arteries end with a musculophrenic artery for the diaphragm and a superior epigastric artery. The latter perforates the rectus sheath and anastomoses in the rectus abdominis muscle with branches of the inferior epigastric artery (branch of the external iliac artery). This anastomosis can bypass blood to the inferior limbs in case of aortic coarctation. In this case, the arterial pulse can be palpated in the rectus abdominis muscle area.
The left internal thoracic artery is situated initially behind the left brachiocephalic vein and in front of the phrenic nerve, descending on the posterior face of the anterior thoracic wall at 0.5–1 cm from the sternum.
Its anterior intercostal branches are accompanied by the intercostal nerve and vein. They perforate the intercostal space under the anterior intercostal membrane. The internal thoracic artery also divides into the pericardiacophrenic and mediastinal branches (Figs. 5.12, 5.13, 5.14 and 5.15).
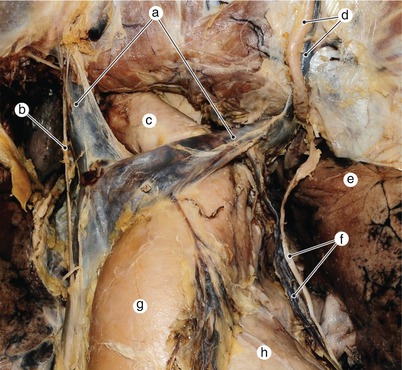
Fig. 5.12




The left internal thoracic artery enters the thorax included between the phrenic nerve and the left innominate vein. Notice the abundance of pericardial veins. a Innominate veins, b right phrenic nerve, c brachiocephalic trunk, d left internal thoracic arteries and veins, e left phrenic nerve and pericardiophrenic vessels, g aorta, h pulmonary trunk
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
