perfusion delivery line and the arterial line (after the systemic pump but before the arterial filter), and arterial and venous inline blood-gas monitors. Temperature-monitoring sites, such as water inflow and outflow for major heat exchangers, venous and arterial blood, cardioplegia solution, and water bath, are also present. A hemoconcentrator is sometimes attached between the systemic flow line, or some other source of blood under pressure, and the venous or cardiotomy reservoir.
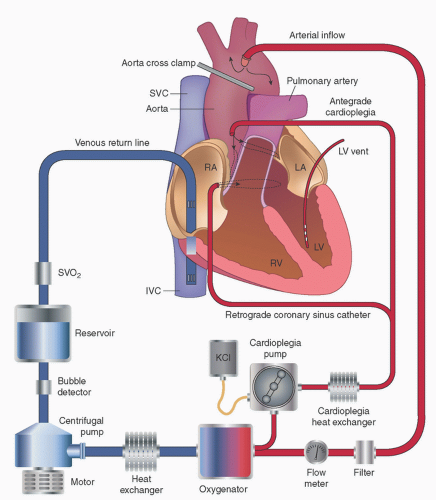 FIGURE 2.1. Simplified extracorporeal circuit diagram. Blood flows by gravity from right atrium and IVC though a cavo-atrial cannula into a venous reservoir. It is then pumped (in this schematic utilizing a centrifugal pump) through a heat exchanger and oxygenator (which are usually integrated as a single membrane oxygenator/heat exchanger) and then through an arterial-line microfilter and is returned to the systemic arterial system (typically the ascending aorta). Also shown are an in-line monitor of venous oxygen saturation, a bubble detector, an arterial-line flow meter, and a cardioplegia delivery system which adds a crystalloid potassium-containing fluid to a source of oxygenated blood, which is then pumped through a separate heat exchanger either into the aortic root (antegrade cardioplegia) or coronary sinus (retrograde cardioplegia). (Redrawn from Miller RD, Pardo MC, eds. Basics of anesthesia. 6th ed. Philadelphia, PA: Elsevier, 2011; used with permission.) |
valve that drains back to the venous or cardiotomy reservoir, a bypass line that goes around the arterial filter in case the latter becomes obstructed, an air bubble detector on the systemic arterial inflow line, and a low-level detector and alarm on the venous reservoir.
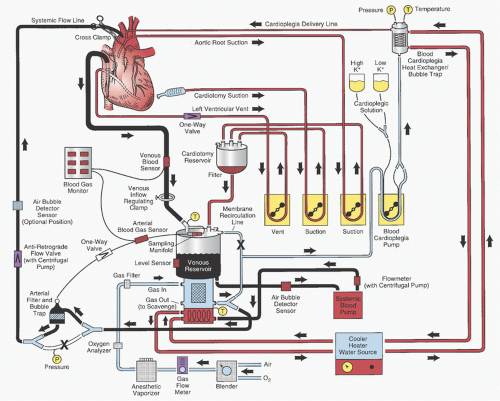 FIGURE 2.2. Detailed schematic diagram of the arrangement of a typical cardiopulmonary bypass circuit using a membrane oxygenator with integral hardshell venous reservoir (lower center) and systemic heat exchanger and external cardiotomy reservoir. Venous cannulation is by a cavo-atrial cannula and arterial cannulation is in the ascending aorta. Some circuits do not incorporate a membrane recirculation line; in these cases the cardioplegia blood source is a separate outlet connector built into the oxygenator near the arterial outlet. The systemic blood pump may be either a roller or centrifugal type. The cardioplegia delivery system (right) is a one-pass combination blood/crystalloid type. The cooler-heater water source may be operated to supply water to both the oxygenator heat exchanger and cardioplegia delivery system. The air bubble detector sensor may be placed on the line between the venous reservoir and systemic pump, between the pump and membrane oxygenator inlet, or between the oxygenator outlet and arterial filter (neither shown), or on the line after the arterial filter (optional position on drawing). One-way valves prevent retrograde flow (some circuits with a centrifugal pump also incorporate a one-way valve after the pump and within the systemic flow line). Other safety devices include an oxygen analyzer placed between the anesthetic vaporizer (if used) and the oxygenator gas inlet and a reservoir level sensor attached to the housing of the hard-shell venous reservoir (on the left). Arrows, directions of flow; X, placement of tubing clamps; P and T (within circles), pressure and temperature sensors, respectively. Hemoconcentrator and Venous cannula (described in text) not shown. |
successful venous drainage. First, the venous reservoir must be below the level of the patient, and second, the lines must be full of blood (or fluid) or else an air lock will occur and disrupt the siphon effect. The amount of venous drainage is determined by the pressure in the central veins (patient’s blood volume), the difference in height between the patient and the top of the blood level in the venous reservoir (negative pressure exerted by gravity equals this height differential in centimeters of water), and the resistance in the venous cannulas, venous line and connectors, and venous clamp, if one is in use.
venous cannula for a patient. For example, a 1.8 m2 body surface area (BSA) patient (total estimated flow, 5.4 L/min; SVC, 1.8 L/min; IVC, 3.6 L/min) at a siphon (gravity) gradient of 40 cmH2O would require at least a 30 French (F) SVC, a 34F IVC, or a single 38F single-stage catheter (8,9). The sizes of two-stage right atrial catheters, based on the BSA of the patient and maximal achievable flow rates, recommended by Shann and Melnitchouk (10) are listed in Table 2.1. Delius et al. (11) offered a method for describing the performance of cannulas used in extracorporeal circulation, called the M number. They reported the M numbers of several different cannulas and provided a nomogram for determining the “M number” and for predicting the pressure gradient across any cannula at any flow based on this number.
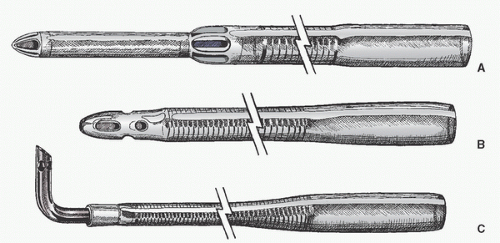 FIGURE 2.3. Drawings of conventional venous cannulas. A: Standard, tapered, two-stage cavo-atrial cannula for insertion into the right atrium (RA) and inferior vena cava (IVC). B: Wire-reinforced cannula for atrial or caval cannulation. C: Cannula with right-angled tip (usually made of metal or hard plastic because the thin wall optimizes the ratio of internal to external diameters). This type of cannula is often used for congenital or pediatric cases and may be inserted directly into the vena cava near its junction with the RA. |
 FIGURE 2.4. Other venous cannulas. (Kaplan JA, Reich DL, Savino JS, et al. Kaplan’s cardiac anesthesia. 6th ed. Philadelphia, PA: Elsevier, 2011, used with permission.) |
TABLE 2.1. Right atrial two-stage cannula, estimated flow rates | |||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||
to make an anastomosis to posterior branches of the circumflex coronary arteries). The cavo-atrial cannula shares many of the advantages of a single right atrial cannula but may provide superior drainage of the right heart, especially in the circumflex position, perhaps by providing some stability to the position of the atrial holes (13).
TABLE 2.2. Comparison of venous cannulation methods | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
atrial cannulas are usually inserted through the right atrial appendage after placing a purse-string suture. Bicaval cannulas may also be placed through incisions in the right atrium or directly into the vena cavae. In the former case, the SVC cannula is usually passed through the right atrial appendage. The IVC cannula is usually passed through a purse-string suture placed in the postero-inferior portion of the lateral wall of the RA near the IVC and avoiding the right coronary artery. The cavo-atrial junctions may be dangerously thin. Often, for bicaval cannulation, surgeons place purse-string sutures directly in the SVC and IVC, but these can cause narrowing when closed.
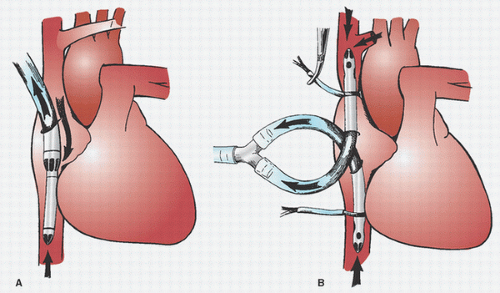 FIGURE 2.5. Methods of venous cannulation: bicaval and cavo-atrial or “two-stage.” A: Single cannulation of right atrium (RA) with a “two-stage” cavo-atrial cannula. This is typically inserted through the right atrial appendage. Note that the narrower tip of the cannula is in the inferior vena cava (IVC), where it drains this vein. The wider portion, with additional drainage holes, resides in the RA, where blood is received from the coronary sinus and superior vena cava (SVC). The SVC must drain through the RA when a cavo-atrial cannula is used. B: Separate cannulation of the SVC and IVC. Note that there are loops placed around the cavae and venous cannulas and passed through tubing to act as tourniquets or snares. The tourniquet on the SVC has been tightened to divert all SVC flow into the SVC cannula and prevent communication with the RA. |
into the RA guided by transesophageal echocardiography (TEE), if available. Specially designed, commercially available (e.g., Medtronic BioMedicus, Inc., Eden Prairie, MN), long, ultrathin, nonkinkable, wire-reinforced catheters are available for this purpose. Insertion may be facilitated by the use of an internal stylet and guidewire. Jones et al. (22) documented flows of up to 3.6 L/min (25F) to 4.0 L/min (27 and 29F) with simple gravity drainage. Using another brand of femoral venous catheter (model Fem-Flex II, Research Medical, Inc.) and gravity drainage, Merin et al. (23) obtained flows of up to 2.5 L/min with 20F catheters and flows of 3.5 to 4.5 L/min with 28F catheters. This flow can be augmented by the use of kinetic or vacuum assistance, which is discussed in the subsequent text. Flow through various femoral venous cannulas augmented by gravity and applied suction have been discussed by Shann and Melnitchouk (10) and are summarized in Table 2.3.
TABLE 2.3. Femoral venous cannula, estimated flow rates | ||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||
noting its passage into the coronary sinus before its arrival into the right atrium. The surgeon should suspect an LSVC when the (right) SVC looks small, and when the left innominate vein is small or absent.
vacuum-assisted system). The negative pressure (or vacuum) measured at this site should not exceed -60 to -100 mmHg (37), but usually -20 mmHg is sufficient. Jones et al. (41) found that vacuum exceeding 40 mmHg increased the amount of GME in a CPB model. It is also desirable to observe the RA directly or through TEE. When the vacuum-assisted system is used, the degree of vacuum applied should be controlled with a vacuum regulator that can be adjusted and can display low levels of suction in 10-mmHg increments. It is important that vacuum should never be applied when there is no forward blood flow through the oxygenator, to prevent air from being pulled across the microporous membrane into the blood path (“bubble transgression”) (42). For this reason and to prevent other causes of air embolization, it is recommended that the venous lines and cannula be filled with fluid, and that vacuum assistance should not be applied until after initiation of CPB. The reservoir should also be open to the atmosphere when vacuum is not being applied to prevent over-pressurization of the venous reservoir with reduction of venous return and risk of retrograde or antegrade air embolization. The venous reservoir should have a low positive (approximately ±5 mmHg) and a high negative (approximately -100 mmHg) pressure relief valve. Usually, adequate venous drainage is achieved with speeds of 1,000 to 1,200 revolutions per minute (rpm) of the kinetic pump or application of 20 mmHg vacuum to the venous reservoir.
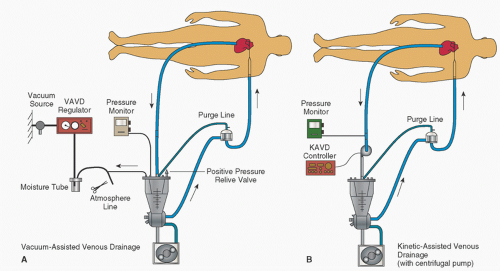 FIGURE 2.6. VAVD and CAVD augmented venous drainage. VAVD, vacuum-assisted venous drainage; CAVD, centrifugal-assisted venous drainage. (Figure 1 from Shann K, Melnitchouk S. Advances in perfusion techniques: minimally invasive procedures. Semin Cardiothor Vasc Anesth 2014;18(2): 146-152,2014;18(2): 146-152, used with permission.) |
lock or can de-prime a centrifugal pump and stop blood flow, or enter the venous reservoir, and can then pass into the arterial circuit and contribute to systemic air embolization and cerebral injury (47,48,49,50). As mentioned earlier, application of an extra ligature around the atrial tissue where the venous cannula exits is advocated to reduce the risk of air aspiration. If vacuum is applied to the closed reservoir system during a no-flow state, there is the theoretic risk of pulling air across the microporous membrane into the blood path, with subsequent systemic air embolism. If the venous reservoir is closed to atmosphere when vacuum is not being applied, the venous reservoir can become overpressurized and reduce venous return while increasing the risk of retrograde or antegrade air embolization (51). If intracardiac septal defects or PFO are present, air pushed into the right heart can lead to massive paradoxical systemic air embolization (49,52). When a pump is being used to augment venous return, there is also a potential for imbalance of flow between the venous drainage and the systemic flow pump, resulting in a change in intravascular volume in the patient or a risk of systemic air embolism. Therefore, the use of assisted venous drainage requires application of special safety monitors and devices, which do not always work (51), and adherence to detailed protocols, and the perfusionist must be even more attentive than when using conventional gravity siphon drainage (1,52). To minimize the risk of retrograde air embolism into the atrium through accidental pressurization of the venous reservoir, it is not prudent to apply vacuum if the venous lines are not full of fluid (as might be done for retrograde autologous priming [RAP]), nor at the time of initiating CPB. It is best to wait until extracorporeal circulation is well established before applying vacuum to the system.
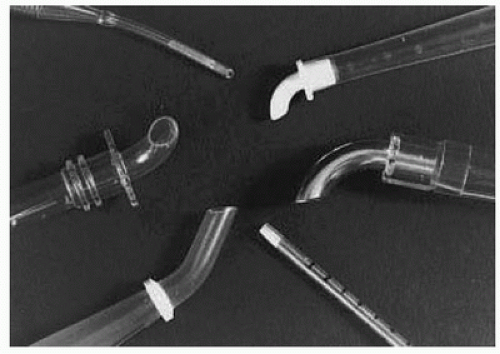 FIGURE 2.7. Conventional arterial cannulas. (From Kaplan JA, Reich DL, Savino JS, et al. Kaplan’s cardiac anesthesia. 6th ed. Philadelphia, PA: Elsevier, 2011, used with permission.) |
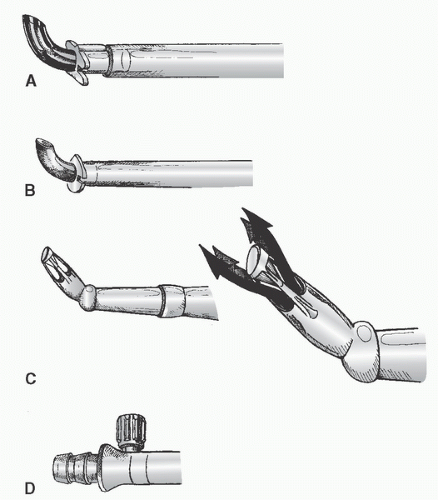 FIGURE 2.8. Other arterial cannulas. A: Metal-tipped right-angled cannula with plastic molded flange for securing cannula to aorta. B: Similar design but with a plastic right-angled tip and molded flange. C: (Left) Diffusion-tipped angled cannula designed to direct systemic flow in four directions to avoid a “jetting effect” that may occur with conventional single-lumen arterial cannulas. An inverted cone occludes the tip. (Right) Drawing with arrows depicts the flow patterns. D: Integral cannula connector and Luer port (for de-airing) incorporated into some arterial cannulas; newer arterial cannulas may contain a self-venting cap (not shown) for removal of air during insertion. |
prototype cannula tip that contains circular lamellae (Stockert Instrumente, Munich, Germany), designed to produce a divergent diffuse flow pattern. These authors compared the hydrodynamics of this new catheter with a standard end-hole cannula (Argyle THI) and the aforementioned Sarns Soft-Flow and Medos X-flow cannulas. The new cannula exhibited the lowest pressure gradient, lowest back-pressure (pressures at various distances and locations beyond the tip), and a broad uniform centric flow dispersion pattern. Reports of clinical studies with the Medos and prototype Stockert arterial cannulas have not been found.
ascending aorta is available), the quality of the aorta, and the surgeon’s preference.
TABLE 2.4. Comparison of arterial cannulation sites | ||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
a small RCT of 60 patients undergoing CABG, found that using an elongated cannula with the tip in the descending aorta, as compared with a short cannula in the ascending aorta, was associated with fewer microembolic signals (TCD), but there was no difference in cognitive performance (seven neuropsychological tests) 9 days postoperatively.
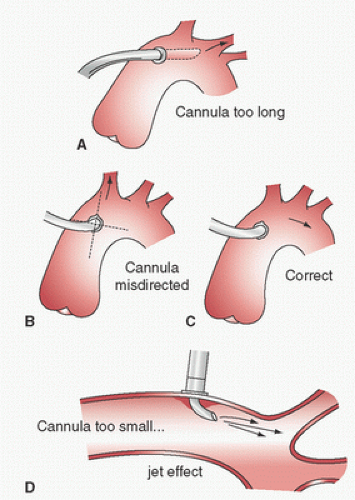 FIGURE 2.9. Aortic cannulation problems. A: cannula extends into carotid owing to excessive length causing excessive carotid flow. B: Cannula is directed into innominate causing hyperperfusion of right carotid and hypoperfusion of left. C: Correct cannula direction. D: Cannula diameter too small; high velocity jet may damage intima or cause decrease flow (venturi effect in some arch branches. (Hensley FA, Martin DE, Gravlee GP, eds. A practical approach to cardiac anesthesia. 5th ed. Philadelphia, PA: Wolters Kluwer, 2013, used with permission.) |
root (because of intramural hematoma), and bleeding from needle or cannulation sites in the aortic root. Subadventitial hematomas tend to be less extensive and softer, and usually resolve when incised. TEE and/or epiaortic ultrasound scanning are useful in diagnosing aortic dissection (93,119,120,121,122).
TABLE 2.5. Ascending aortic dissection complicating cardiac surgery | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
plication (118), but such repairs may fail early or later and therefore graft replacement is generally favored (124,120). Survival of those cases recognized and treated in the operating room has ranged from 66% to 85%. When not recognized until postoperatively, survival has been 50% or less (Table 2.5).
TABLE 2.6. Femoral artery cannula, estimated flow rates | |||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||
limited-access surgery and has been complicated by fatal dissection (143,144,145). Galloway et al. (141) reported an arterial dissection rate of approximately 0.8% in a registry of 1,063 patients undergoing retrograde femoral cannulation and CPB with a port-access system (HeartPort, Inc., Redwood City, CA), whereas Grossi et al. (145b) reported a rate of 0.3% in a single-center experience with 714 patients undergoing minimally invasive mitral valve surgery. (In 564 of these patients, arterial cannulation was into the femoral artery.)
vessel hydrodynamics have been demonstrated during perfusion through the right subclavian artery in a mock circulation (163); however, the absence of subclavian artery stenosis should first be documented by comparing noninvasive or invasive arterial pressure in each arm (164) before choosing this route.
 FIGURE 2.10. Cannulation of right subclavian artery. (Figure 1 from Di Luozzo G, Griepp R. Cerebral protection for aortic arch surgery: deep hypothermia. Semin Thoracic Surg 2012; 24:127-130, used with permission.) |
sternotomy in 30 patients and a separate neck incision in 70. They attached an 8- to 10-mm vascular graft end-to-side to the carotid artery during a period of carotid cross-clamping, through which the arterial cannula was inserted. They also used this cannula to provide selective unilateral antegrade cerebral perfusion during circulatory arrest. This group has also used the right common carotid artery for arterial annulation (193,194).
TABLE 2.7. Priming volume and maximum flow rates for various-sized tubing | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
standards and has met the test of time for several decades. However, some of the plasticizers used (e.g., di-(2)-ethylhexyl-phthalate [DEHP] and bisphenol A [BPA]) may have bioincompatibility. Therefore, the search for better materials continues. Polyolefin is a possible alternative to PVC and has the advantage of containing no plasticizers and therefore is nontoxic and noninflammatory. However, widespread use is hampered by its relatively high cost (203). Silicone rubber and latex rubber tubing were sometimes used in roller pumps in the past; however, spallation and blood incompatibility were problematic. New formulations of PVC that minimize spallation are being developed for use in roller pumps.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


