Home BP
Office BP
Ambulatory BP
Number of BP measurements
++
+
+++
Misleading phenomena (white-coat effect, masked hypertension effect, placebo effect)
−
+
−
Observer bias elimination
+++ (automated devices
or telemonitoring)
+
+++
Reproducibility
+++
+
+++
Study power and sample size
+++
+
+++
Subjects selection
+++
+
+++
Diagnosis of true resistant hypertension
++
+
+++
Assessment of treatment-induced BP changes
++
+
+++
Assessment of treatment-induced changes in organ damage
++
+
+++
Assessment of morning hypertension
+++
+
+++
Assessment of nocturnal hypertension
++ (specific
devices)
−
+++
Assessment of variability
– Short-term
−
−
++
– Mid-term
++
−
−
– Long-term
++
++
−
Association with preclinical organ damage
+++
+
+++
Association with cardiovascular events risk
+++
+
+++
Compliance with drug treatment
+++
+
+
Patients’ preference
+++
+
+
Guidance in hypertension management
++
+
++
Repeated monitoring in longitudinal trials
+++
++
+
Cost-effectiveness
+++
++
+
10.2 Advantages of HBPM for Clinical Research
HBPM has major advantages in clinical research. As with ABPM, HBPM provides multiple readings in the individual’s usual environment. However, home measurements may be obtained over several days, weeks, or even months, whereas ABPM is typically conducted during a 24-h period and cannot be repeated more frequently than 2 or 3 times in a trial. On the contrary, office BP monitoring (OBPM) obtains a few readings, typically taken in the clinical environment which is a potentially stressful setting that promotes the emergence of the white-coat effect, masked hypertension, placebo effect, and observer bias [2]. Hence, HBPM and ABPM have advantages that result in superior reproducibility and diagnostic accuracy compared to conventional office BP measurements [3]. Regarding prognostic significance, HBPM has demonstrated close associations with several manifestations of early target organ damage and cardiovascular events risk, which are superior to those obtained by OBPM and similar to those by ABPM [4, 5]. In addition, HBPM is more acceptable to patients than ABPM, since it causes only minimal restriction of daily activities and no interruptions during sleep [6]. HBPM has been also shown to improve patients’ compliance with drug treatment and hypertension control rates [2].
10.3 Implications of HBPM in Clinical Research
10.3.1 Selection of Study Participants
Τhe selection of appropriate study participants is one of the most important methodological issues in clinical hypertension research. HBPM is a valuable diagnostic tool that accurately defines hypertension phenotypes in studies aiming to investigate the prevalence, characteristics, determinants, and prognostic significance of a specific BP pattern. In addition, isolation of BP patterns such as white-coat and masked hypertension that may exhibit heterogenous behavior and distort findings of a study is needed by out-of-office monitoring. For example, in study participants with white-coat hypertension, there is often minimal ambulatory BP response to antihypertensive drug therapy compared to those subjects with sustained hypertension [9]. Studies in patients with resistant hypertension also have demonstrated the importance of using HBPM for the reliable diagnosis and the exclusion of the white-coat hypertension phenomenon, which is common even among treated and moderately to severely hypertensive subjects [10, 11].
10.3.2 Improvement of Study Power and Reduction of Sample Size
The reproducibility of a BP measurement method, expressed as the standard deviation of differences between repeated measurements, plays a major role in the calculation of the sample size required for a clinical trial. As has been observed with ABPM, HBPM also has superior reproducibility to OBPM which makes it useful for clinical trials that compare the efficacy of antihypertensive drugs since it allows the same antihypertensive effect size to be identified with higher precision [3]. In other words, HBPM allows a smaller sample size to be recruited in order to identify a difference in the BP lowering effect of two drugs with the same study power [3, 12].
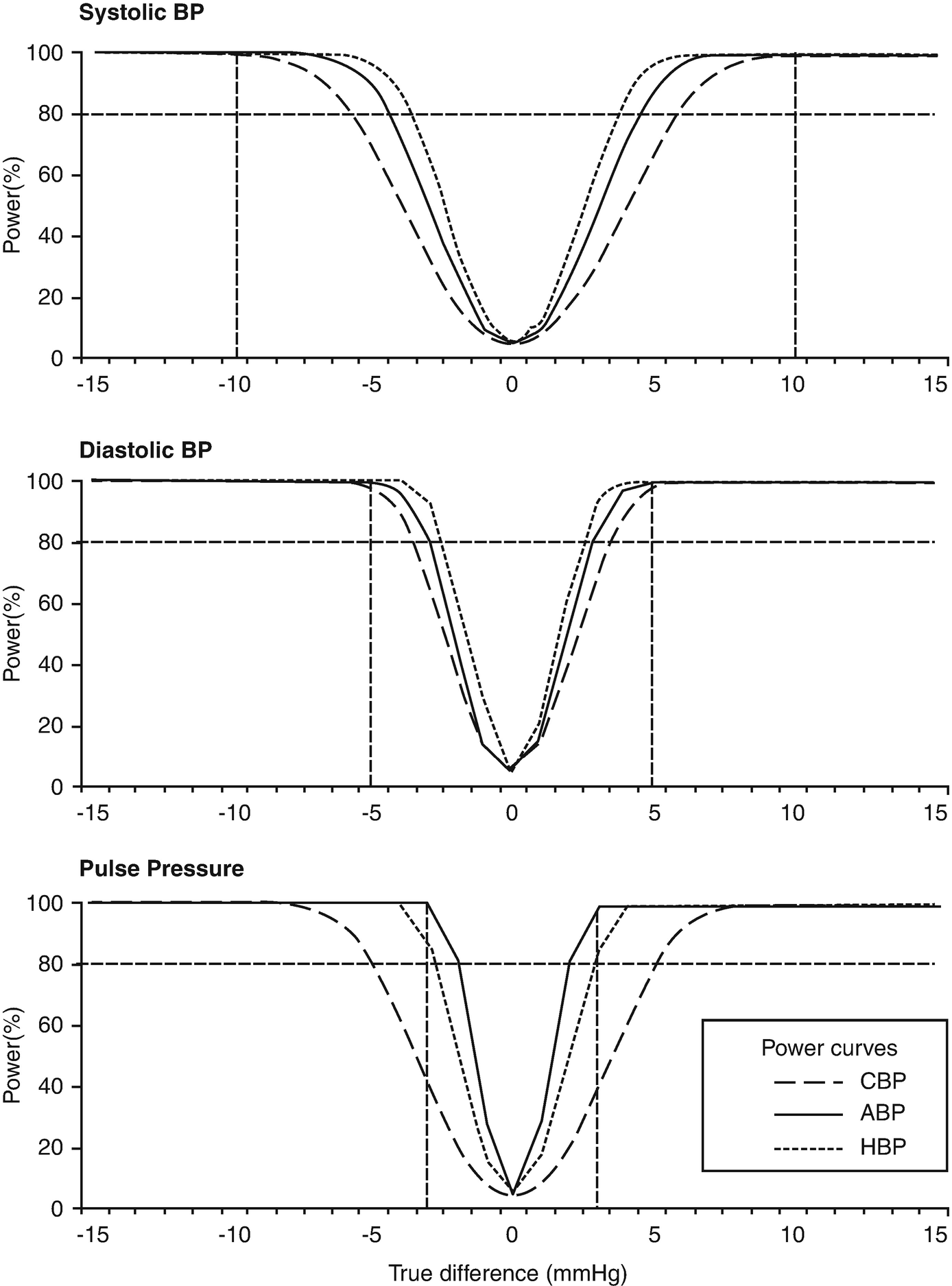
Study power curves of a randomized crossover clinical trial comparing the efficacy of two antihypertensive drugs using blood pressure measurements in the clinic, at home and with ambulatory monitoring (from [13]). BP blood pressure, CBP clinic BP, ABP 24-h ambulatory BP, HBP home BP. Horizontal dotted lines indicate 80% power to detect a difference in the hypotensive effect of the drugs of 10 mmHg for systolic, 5 mmHg for diastolic BP, or 3 mmHg for pulse pressure (vertical dotted lines)
10.3.3 Evaluation of the Effects of Antihypertensive Drugs
10.3.3.1 Evaluation of the Magnitude of BP Lowering Effect
Because of its superior reproducibility to OBPM, HBPM provides a more accurate classification of the true baseline BP and improves the precision for the determination of antihypertensive drug treatment-induced BP changes. These benefits are also related to the absence of the placebo effect, regression dilution bias (regression to the mean), and observer bias (when electronic devices with automated memory are used), which typically affect clinical trials when OBPM is employed.
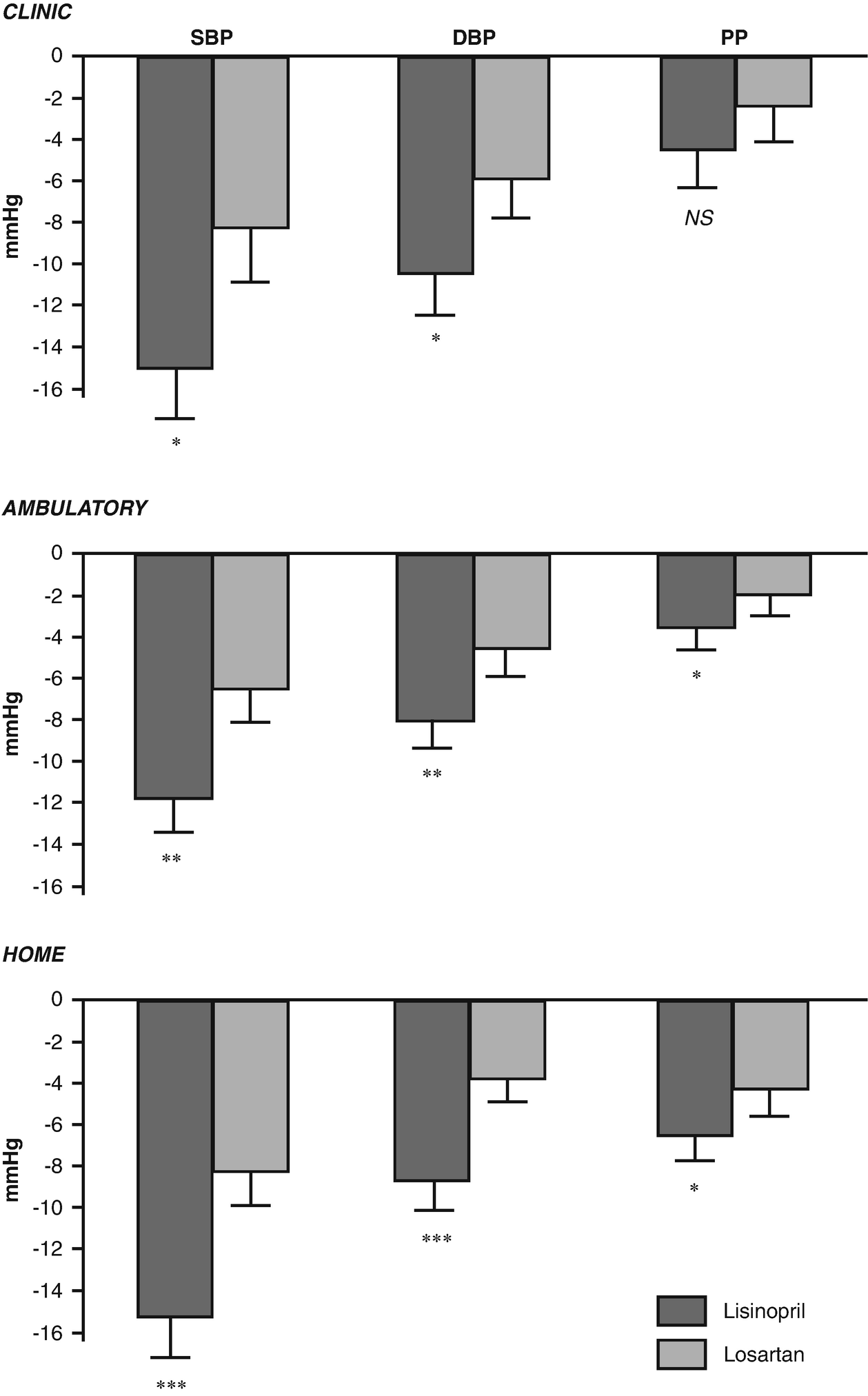
Randomized crossover comparative clinical trial of the effects of two antihypertensive drugs on clinic, 24-h ambulatory and home blood pressure (from [13]). SBP systolic blood pressure, DBP diastolic blood pressure, PP pulse pressure, ∗, P < 0.05; ∗∗, P < 0.01; ∗∗∗, P < 0.001 for differences between the two drugs)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


