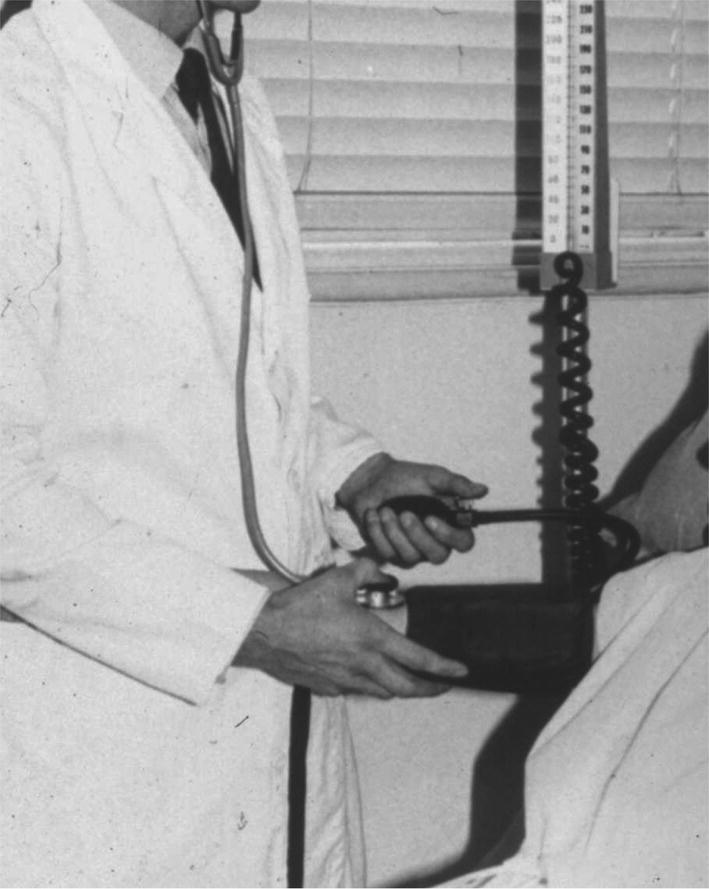
Chapter 4 Traditionally, blood pressure has been assessed with the auscultatory technique introduced into clinical medicine at the end of the nineteenth century. Despite being prone to inaccuracy because of inattention to the requirements needed to obtain accurate measurement, this technique has survived largely unchanged for over 100 years. It is salutary to reflect that since Riva-Rocci and Korotkoff introduced the technique, we have landed men on the moon, encircled Mars, invented the automobile and airplane and, most importantly, revolutionised the technology of science with the microchip. Clinical practice has been criticised for ignoring scientific evidence and thereby perpetuating a measurement technique that is likely to be misleading. However, this criticism has been addressed with publication of the recommendations of the National Institute of Clinical Excellence (NICE) in August 2011, which states that ambulatory blood pressure measurement ‘should be implemented for the routine diagnosis of hypertension in primary care’ (Figure 4.1). Figure 4.1 NICE guideline. The NICE recommendation is based not only on the large irrefutable evidence base that ambulatory blood pressure measurement is superior to all other measurement techniques for the diagnosis and management of patients with hypertension but also on the fact that it been shown to be a more cost-effective technique than either conventional measurement or self-measurement of blood pressure. An accurate device is fundamental to all measurements of blood pressure. If a device is inaccurate, attention to the detail of measurement methods is of little relevance. The accuracy of devices for measurement of blood pressure should not be judged on the sole basis of claims from manufacturers, which can be extravagant. Instead devices should be validated according to international protocols in peer-reviewed journals. A number of websites provide updated assessments of all devices used to measure blood pressure and indicate which have passed or failed independent validation. No matter which measurement device is used, blood pressure is always a variable haemodynamic phenomenon. Modification of the factors that influence variability is not always possible, but we can minimise their effect. When optimum conditions are not possible, this should be noted with the reading. White coat hypertension is a condition where people with normal blood pressure outside the medical environment have hypertension during measurement by doctors and nurses. White coat hypertension is shown best by ambulatory blood pressure measurement. This phenomenon, which occurs in both treated and untreated subjects, is present when the office blood pressure is higher than self-measured blood pressure and/or the daytime ambulatory blood pressure but the latter is also above normal. These white coat phenomena are important because a decision to initiate drug treatment or to modify drug dosage should never be made on the basis of conventional measurement of blood pressure. Posture affects blood pressure, with a general tendency for it to decrease when a person moves from the lying position to the sitting or standing positions. Some patients may have postural hypotension, especially those who are taking certain antihypertensive drugs and elderly people. When this is likely, blood pressure should also be measured when the patient is standing, but ambulatory blood pressure measurement is the most effective way of diagnosing symptomatic hypotension. If the arm in which blood pressure is being measured is unsupported – as tends to happen when the patient is sitting or standing – the patient will perform isometric exercise, which can increase blood pressure by as much as 10%. The arm therefore must be supported during measurement of blood pressure, especially when the patient is in the standing position. This is achieved best in practice by the observer holding the patient’s arm at the elbow (Figure 4.2). Figure 4.2 Arm support during blood pressure measurement. The forearm should be at the level of the heart – that is, the mid-sternum. Measurement in an arm lower than the level of the heart leads to an overestimation of systolic and diastolic pressures, while measurement in an arm above the level of the heart leads to underestimation. Such inaccuracy can be as much as 10 mm Hg, especially when the patient is in the sitting or standing position, when the arm is likely to be below heart level by the side. Arm position is important for self-measurement of blood pressure, especially with devices for wrist measurement. Arterial disease can cause differences in blood pressure between arms, but because blood pressure varies from beat to beat, any differences may simply reflect blood pressure variability or measurement errors, or both. Bilateral measurement should be made at the first consultation; if differences >20 mm Hg for systolic or 10 mm Hg for diastolic blood pressure are present on consecutive readings, the patient should be referred to a cardiovascular centre for further evaluation with simultaneous bilateral measurement and for the exclusion of arterial disease (Figure 4.3). Figure 4.3 Which arm? Crossing legs has been shown to increase blood pressure and when measurement is made both feet should be flat on the floor with the legs uncrossed. The cuff is an inelastic cloth that encircles the arm and encloses an inflatable rubber bladder. The cuff is secured around the arm most often by means of Velcro on the adjoining surfaces of the cuff. Velcro surfaces must be effective; when they lose their grip, the cuff should be discarded. It should be possible to remove the bladder so that the cuff can be washed. All devices in clinical use are dependent on cuff occlusion of the arm and are prone to the inaccuracy of miscuffing. Firstly, a bladder that is too long for the arm may result in underestimation of blood pressure, but more commonly, a bladder that is too short and does not encircle the arm will overestimate blood pressure – so-called cuff hypertension. Miscuffing is a serious source of error that leads inevitably to incorrect diagnosis in clinical practice and erroneous conclusions in research into hypertension. Whatever cuff is used, the centre of the bladder should be placed over the brachial artery, to minimise the occurrence of cuff hypertension (Figure 4.4). Figure 4.4 Placement of cuff. Many national bodies now recommend a range of cuffs to cater for all eventualities, which presupposes that the user will measure the arm circumference and, having done so, will have access to an adequate range of cuffs. In practice, neither of these requirements is easily fulfilled. Societies differ in their recommendations. The striking difference between the American and British recommendations is not so much the length of the bladders but the width: most European arms will comfortably accommodate a bladder with a width of 12 cm, but a bladder with a width of 16 cm is likely to encroach on the antecubital fossa – particularly if (as often happens in practice) the sleeve of the patient’s shirt or blouse is rolled up. Certain groups of people merit special consideration for the measurement of blood pressure because of age, body habitus or disturbances of blood pressure related to haemodynamic alterations in the cardiovascular system. Measurement of blood pressure in children presents a number of difficulties. Variability of blood pressure is greater than in adults, and any one measurement is less likely to represent the true blood pressure. Systolic pressure is more accurate and reproducible than diastolic pressure. A cuff with proper dimensions is essential for accurate measurement. The widest cuff practicable should be used. Ideally, blood pressure should be measured after a few minutes of rest. Values obtained during sucking, crying or eating will not be representative. As with adults, a child’s blood pressure status should be decided only after it has been measured on a number of separate occasions. Ambulatory blood pressure measurement is being used increasingly in children. In epidemiological and interventional studies, blood pressure predicts morbidity and mortality in elderly people as effectively as in the young. Elderly people have considerable variability in blood pressure, which can lead to a number of diurnal blood pressure patterns that are identified best with ambulatory blood pressure measurement. These patterns include isolated systolic hypertension, white coat hypertension and hypotension. Elderly patients may also have pseudohypertension, a condition in which there is a large discrepancy between cuff and direct measurement of blood pressure in elderly patients. When conventional measurements seem to be out of proportion with the clinical findings, referral to a specialist cardiovascular centre for further investigation may be an appropriate option. The association between obesity and hypertension has been confirmed in many epidemiological studies. Obesity may affect the accuracy of measurement of blood pressure in children, young and elderly people, and pregnant women. The relation of arm circumference to bladder dimensions is particularly important. If the bladder is too short for the arm as often happens with obese arms, blood pressure will be overestimated – ‘cuff hypertension’. The increasing prevalence of the metabolic syndrome (obesity, hypertension and hyperglycaemia) makes accurate measurement of blood pressure in obese people increasingly important. In some obese patients, the arm circumference is so great that upper arm measurement is not possible and forearm measurement may be the only option. For conventional measurement, the Korotkoff sounds are auscultated over the radial artery and for devices that measure blood pressure by oscillometry (devices for self-measurement and ambulatory blood pressure measurement), the cuff is placed on the forearm. Large variations in blood pressure from beat to beat make it difficult to obtain accurate measurements in patients with arrhythmias. In patients with arrhythmias, such as atrial fibrillation, blood pressure varies depending on the preceding pulse interval. No generally accepted method of determining auscultatory end points in patients with arrhythmias exists. Devices for measuring blood pressure with oscillometry vary in their ability to accurately record blood pressure in patients with arrhythmias. Measurements of blood pressure at best will constitute a rough estimate in those with atrial fibrillation, particularly when the ventricular rhythm is rapid or highly irregular, or both. The rate of deflation should be no faster than 2 mm Hg per heartbeat, and repeated measurements may be needed to overcome variability from beat to beat (Figure 4.5). Figure 4.5 Atrial fibrillation. Two potential sources of error exist when patients have bradyarrhythmia. If the rhythm is irregular, the same problems as with atrial fibrillation will apply. When the heart rate is extremely slow – for example, 40 beats/min – it is important that the rate of deflation used is less than for people with normal heart rates, as too rapid deflation will lead to underestimation of systolic blood pressure and overestimation of diastolic blood pressure. Clinically, relevant hypertension occurs in more than 10% of pregnant women in most populations. High blood pressure is a key factor in making medical decisions in pregnancy. Disappearance of sounds (fifth phase) is the most accurate measurement of diastolic pressure, except when sounds persist to zero, in which case the fourth phase of muffling of sounds should be used. In patients who take antihypertensive drugs, the timing of measurement may have a substantial influence on the blood pressure. The time of taking antihypertensive drugs should be noted. Systolic blood pressure increases with increasing dynamic work as a result of increasing cardiac output, whereas diastolic pressure usually remains about the same or moderately lower. An exaggerated blood pressure response during exercise may predict development of future hypertension. The advancing development of technology is likely to bring further innovative changes in blood pressure measurement. The term ‘conventional blood pressure measurement’ is open to misinterpretation unless clearly defined. It is sometimes applied to the traditional auscultatory technique of blood pressure measurement using a stethoscope and mercury sphygmomanometer, whereas it can also be applied to any method of measurement used in the setting of clinical practice. For the purpose of this book, it is the measurement of blood pressure by whatever means in a medical setting, such as a doctor’s office or surgery, a hospital clinic or outpatient department, or a pharmacy. It is distinguished, therefore, from what are often referred to as ‘out-of-office’ measurements, such as self-measurement or ambulatory blood pressure measurement. Conventional measurement of blood pressure will remain the initiating measurement technique for most patients. However, accurate automated devices, some of which can give repeated measurements and thereby minimise the likelihood of misdiagnosis, are replacing the auscultatory technique. Conventional measurement of blood pressure with a mercury sphygmomanometer and stethoscope, which was first introduced to medicine by Scipione Riva-Rocci and Nicolai Korotkoff at the end of the nineteenth century, is now used decreasingly in clinical practice for a number of reasons (Figure 4.6). Figure 4.6 Riva-Rocci sphygmomanometer. Source: Reproduced with permission from O’Brien, E. & Fitzgerald, D. (1991) The history of indirect blood pressure measurement. In: Blood Pressure Measurement (eds E. O’Brien & K. O’Malley). Elsevier, Amsterdam. © Elsevier. However, apart from what might be termed a sentimental desire to retain a century-old method that is the last measurement technique used regularly in clinical examination, there are two reasons why the technique should be retained. Firstly, in patients with arrhythmias, blood pressure measurement with automated techniques may not be possible, and in this circumstance the average of a number of auscultatory measurements may be the best estimate of blood pressure. Secondly, in some patients it is not possible (for reasons that are not apparent) to measure blood pressure with oscillometric techniques and the auscultatory technique has to be used. The mercury sphygmomanometer is a simple, accurate and reliable device that can be serviced easily, but concerns rightly exist about the toxicity of mercury for people who use mercury sphygmomanometers and those who service them. The greatest concern about mercury, however, is its toxic effect on the environment, and mercury increasingly is being banned from use in medicine. Alternative devices to the mercury sphygmomanometer, which combine the features of electronic and mercury devices by using an electronic pressure gauge as a substitute for the mercury column, are now available. These devices, which are known as hybrid sphygmomanometers, display cuff pressure as a simulated mercury column with a digital readout on a liquid crystal display. An aneroid scale may be used instead of a mercury-like column. The cuff is deflated in the normal way; when systolic and diastolic pressure are heard, a button next to the deflation knob is pressed, which freezes the digital display to show systolic and diastolic pressures. This offers the potential of eliminating terminal digit preference, which is a major problem with the clinical use of any auscultatory monitor. The observer is therefore able to measure blood pressure with the traditional auscultatory technique without necessarily having to rely on automated readings. This is achieved without the risk of mercury toxicity (Figure 4.7). Figure 4.7 Hybrid sphygmomanometer. Source: Reproduced with permission from A&D Company. Aneroid sphygmomanometers register pressure through a bellows and lever system that is more intricate mechanically than the mercury reservoir and column. The jolts and bumps of everyday use affect accuracy over time, which usually leads to falsely low readings and thus underestimations of blood pressure. They are therefore less accurate in use than mercury or hybrid sphygmomanometers. As mercury sphygmomanometers are removed from clinical practice, they are often replaced with aneroid devices on the false assumption that they are equally accurate. Remarkably little literature exists on the accuracy of aneroid devices and what does is generally negative. All sphygmomanometric methods that are dependent on the auscultatory technique are prone to all the problems of observer inaccuracy. The major cause of observer error is the variability of blood pressure and the misleading measurements that constitute the phenomenon of white coat hypertension and masked hypertension may now be added to this list. Training of observers in the technique of auscultatory measurement of blood pressure is often taken for granted. Instruction to medical students and nurses has not always been as comprehensive as it might be, and assessment for competence in the measurement of blood pressure has been a relatively recent development. A number of training methods exist; they include: direct instruction with a binaural or multi-aural stethoscope; manuals, booklets and guidelines; electronic instruction in which the trainee can be assessed by visually watching a falling mercury and listening to Korotkoff sounds. The inflation–deflation system consists of an inflating and deflating mechanism connected by rubber tubing to an occluding bladder. The standard mercury, hybrid and aneroid sphygmomanometers used in clinical practice are operated manually, with inflation by means of a bulb compressed by hand and deflation by means of a release valve, which is also controlled by hand. The pump and control valve are connected to the inflatable bladder and to the sphygmomanometer. One of the most common sources of error in sphygmomanometers is the control valve. A stethoscope should be of high quality, with clean and well-fitting earpieces. Whether the bell or diaphragm is used in routine measurement of blood pressure probably does not matter much, as long as the stethoscope is placed over the palpated brachial artery in the antecubital fossa. As the diaphragm covers a larger area and is easier to hold than a bell end piece, it is reasonable to recommend it for routine clinical measurement of blood pressure. Electronic stethoscopes that amplify the Korotkoff sounds are now commonly used in clinical practice. To check and maintain mercury sphygmomanometers is easy, but great care should be taken when mercury is handled. Mercury sphygmomanometers need cleaning and checking at least every 6 months in hospital use and every 12 months in general use. In practice, doctors often neglect to have sphygmomanometers checked and serviced. The responsibility for reporting faulty equipment or lack of appropriate cuffs lies with the observer, who should always refuse to use defective or inappropriate equipment. Aneroid and hybrid sphygmomanometers should be checked every 6 months against an accurate mercury sphygmomanometer over the entire pressure range. If inaccuracies or other faults are found, the instrument should be repaired by the manufacturer or supplier. The major source of inaccuracy in the technique is observer error. Observers should be trained in the auscultatory technique and should have good hearing. The observer should take care to position the manometer so that the scale can be read easily. Accurate measurement is achieved most effectively with stand-mounted models, which can easily be adjusted to suit the height of the observer (Figure 4.8). The mercury manometer has a vertical scale, and errors will occur unless the eye is level with the meniscus. The aneroid scale is a composite of vertical and horizontal divisions and numbers, and it must be viewed straight on, with the eye on a line perpendicular to the centre of the face of the gauge. Figure 4.8 Eye level. The cuff should be wrapped around the arm, ensuring that the dimensions of the bladder are accurate. If the bladder does not completely encircle the arm, the centre of the bladder must be over the brachial artery. The rubber tubes from the bladder are usually placed inferiorly, often at the site of the brachial artery, but placing them superiorly allows easy access to the antecubital fossa for auscultation. The lower edge of the cuff should be 2–3 cm above the point of brachial artery pulsation (Figure 4.9). Figure 4.9 Cuff placement. The brachial artery should be palpated while the cuff is inflated rapidly to about 30 mm Hg above the point where the pulse disappears; the cuff is then deflated slowly, and the observer notes the pressure at which the pulse reappears. This is the approximate level of the systolic pressure. Palpatory estimation is important, because phase I sounds sometimes disappear as pressure is reduced and reappear at a lower level (the auscultatory gap), which results in systolic pressure being underestimated unless already determined by palpation. The palpatory technique is useful in patients in whom auscultatory end points may be difficult to judge accurately, for example, pregnant women, patients in shock and those who are exercising. (The radial artery is often used for palpatory estimation of the systolic pressure but use of the brachial artery also allows the observer to establish its location before auscultation begins.) For many years, recommendations on blood pressure measurement have been uncertain about the diastolic end point – the so-called diastolic dilemma. Phase IV (muffling) may coincide with or be as much as 10 mm Hg higher than phase V (disappearance), but usually the difference is less than 5 mm Hg. Disappearance of sounds (phase V) should be taken as diastolic pressure. When the Korotkoff sounds persist down to zero, muffling of sounds (phase IV) should be recorded for diastolic pressure, and a note made to this effect. To make measurement of conventional blood pressure more informative and accurate, it is important to record the circumstances of measurement as well as the levels of blood pressure recorded. Reliability of measurement is improved if repeated measurements are made and measurement of ambulatory blood pressure or self-measurement of blood pressure, or both, give much valuable information that cannot be obtained with measurement of conventional blood pressure. Automated devices that are dependent on the oscillometric method for measuring blood pressure are replacing the auscultatory technique. They are being used increasingly in office, clinics and hospitals across the world. The oscillometric method measures mean blood pressure, and a specific algorithm (known only to the manufacturer) estimates systolic and diastolic blood pressure. Automated devices for blood pressure measurement should be validated independently using one of the internationally accepted validation protocols. The most commonly used protocol is the European Society of Hypertension International Protocol (ESH-IP). Several oscillometric devices for professional use have been validated and are available on the market. Overall, automated devices are superior to auscultatory measurement of blood pressure, but they also have limitations. Some professional oscillometric devices have been programmed to take multiple blood pressure readings in the office or clinic (by manual activation or bluetooth), which allows measurements to be obtained in the absence of an observer, while patients are alone in the examination room (automated office blood pressure measurement). Such devices minimise the office reaction (white coat effect) and give blood pressure values that are closer to those obtained by daytime ambulatory blood pressure monitoring.
Blood pressure measurement
Part I: Factors influencing all techniques of blood pressure measurement
Advances in technology and blood pressure measurement
Selection of an accurate device
Variability of blood pressure
White coat hypertension
White coat effect
Posture
Arm support
Arm position
Which arm?
Crossing legs
Cuff and bladder
Cuff hypertension
Special management of blood pressure
Children
Elderly people
Obese people
Patients with arrhythmias
Pregnant women
Patients who take antihypertensive drugs
Patients who are exercising
The impact of future technological advances
Further Reading
Part II: Conventional blood pressure measurement
Definition
The auscultatory technique of blood pressure measurement

Sphygmomanometers for auscultatory measurement
Mercury Sphygmomanometers
Hybrid sphygmomanometers

Aneroid sphygmomanometers
Problems common to all methods of auscultatory measurement
Observer inaccuracy
Inflation–deflation system
Stethoscope
Maintenance
Performing auscultatory measurements
Observer skill
Position of manometer
Placement of cuff
Palpatory estimation of blood pressure
Diastolic dilemma
Recording blood pressure
Automated blood pressure measurement
Sphygmomanometers for automated measurement
Oscillometric methodology
Accuracy of automated devices
Advantages and disadvantages of automated measurement
Further Reading
Part III: Ambulatory blood pressure measurement
Blood pressure measurement
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


