Benign Neoplasms
Keith M. Kerr FRCPath
Benign neoplasms of the lung are numerous, heterogeneous, and rare. Most occur in the lung periphery, neither visible to the bronchoscopist nor likely to be sampled by bronchial biopsy. Transbronchial biopsy could access a tiny portion of tumor tissue, but in all but the most exceptional case, it is highly unlikely that material will be obtained exhibiting sufficient features to allow a specific diagnosis. Some benign lung tumors do involve more central bronchi and may be encountered at bronchoscopy. These include squamous cell papilloma, glandular papilloma or mixed lesions, mucous gland adenoma, pleomorphic adenoma, chondroid hamartoma, and lipoma.
Squamous cell papillomas are mostly exophytic lesions but may be inverted, and they are usually solitary in adult men. The bronchi may be involved by multiple papillomas in juvenile laryngotracheal papillomatosis. Biopsy shows well-differentiated stratified squamous epithelium covering a loose fibrovascular stroma. Some keratinize, others show transitional epithelium, and 20% show koilocytosis. Dyskeratosis, focal atypia, and mitoses occur, and caution must be taken to distinguish them from well-differentiated squamous cell carcinoma. Glandular and mixed lesions are exceptionally rare. The glandular epithelium may be ciliated, mucigenic or mixed, pseudostratified, or simple columnar.
Mucous gland adenoma is extremely rare and comprises glands, tubules, and cystic mucin-filled spaces lined by cytologically bland cuboidal, columnar, or flattened cells, and occasionally papillae. As with other bronchial tumors, the overlying mucosa may show squamous metaplasia. Definitive diagnosis usually requires an excision specimen.
Biopsy of pleomorphic adenoma may reflect the biphasic nature of this lesion with fibromyxoid stroma and sheets or cords of epithelial and/or myoepithelial cells. Glands and chondroid stroma are less common.
Chondroid hamartoma, also referred to as mesenchymoma, is endobronchial in 10% of cases. Lesions comprise a variable mixture of mature cartilage, fat (common in endobronchial lesions), connective tissue, smooth muscle, and even bone, together with bland epithelial cell-lined cleft-like spaces. In biopsy samples the challenge is to recognize the abnormal disposition and quantity of elements that are otherwise normal bronchial constituents. The cartilage is more cellular than normal but not atypical. Lipoma, possibly related to hamartoma, comprises only mature adipocytes and, rarely, occasional lipoblast-like cells.
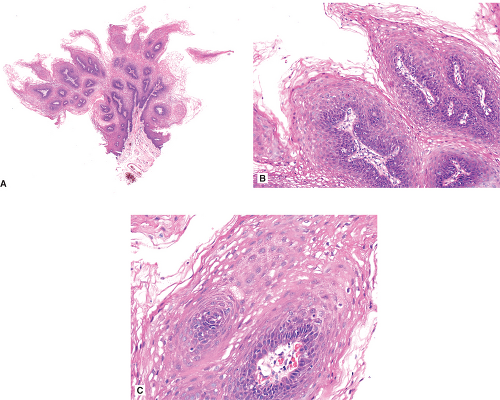 Figure 8.1: (A) Low power of squamous cell papilloma biopsy. The papillary pattern can be appreciated. (B) Thin fronds of squamous cell papilloma lined by a bland squamous epithelium. (C) High power shows well-differentiated stratified squamous epithelium covering a loose fibrovascular stroma.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|