Chapter 68 Benign Lung Tumors*
Classification
Benign neoplastic tumors are classified histologically according to the World Health Organization (WHO) classification updated in 2004 (Box 68-1). These histologic distinctions are more helpful to the pathologist than to the clinician approaching a lung tumor and are more likely to be in the “is it malignant or not” mindset. Although typically benign, many of the benign neoplasms have the potential for malignant transformation.
Benign Epithelial Neoplasms
Papillomas
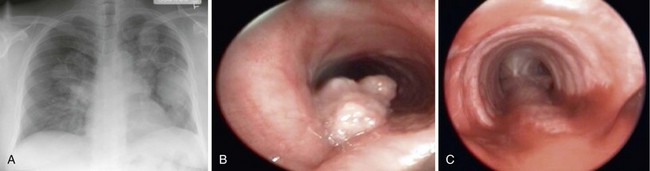
Benign epithelial neoplasms are generally rare, although squamous papilloma is the most common. Histologically, these are identified as papillary tumors with a squamous cell epithelial surface and delicate connective tissue attachments. They may be solitary or multiple and most often occur in the larynx and trachea, with less than 10% having lower airway involvement and only 2% within the lung parenchyma (Figure 68-1). The squamous type of papilloma has an association with human papillomavirus (HPV types 16, 18, 31, 33, and 35). Obstructive symptoms may develop from airway involvement and are an indication for laryngoscopic or bronchoscopic removal. Recurrent papillomas occur in as many as 20%, and some patients require periodic endoscopic debridement. Malignant transformation to squamous cell carcinoma may occur. Compared with squamous cell papillomas, glandular and mixed-cell papillomas are exceedingly rare.