Bacterial Pneumonia
Pneumonia is a common cause of morbidity and mortality. In the United States there are an estimated 4 million cases of community-acquired pneumonia annually, resulting in approximately 600,000 hospitalizations (1,2). A meta-analysis of the prognosis and outcome of 33,148 patients who had community-acquired pneumonia showed an overall mortality rate of approximately 14% (3). The mortality varies considerably in specific groups of patients. The mortality rate in patients not requiring hospitalization is approximately 0.1% (1). However, reported mortality rates in patients who have pneumonia of sufficient severity to require hospitalization range from 4% to almost 40% (3,4,5). Pneumonia develops in approximately 0.5% to 1.0% of hospitalized patients (nosocomial pneumonia) (6). Mortality in such patients is higher, being estimated at approximately 30% (7,8). In one prospective multicenter study of 2,402 patients in intensive care units (ICUs), 163 (6.8%) of the patients developed nosocomial pneumonia; 75.5% (n = 123) of all patients with nosocomial pneumonia were on assisted ventilation (9). One hundred sixty three patients, who were admitted to the ICU during the same period but had no evidence of pneumonia, were used as a control group. For the patients with pneumonia the mean length of stay in the ICU and hospital was significantly longer than in controls, and their mortality five times greater (9).
A diagnosis of pneumonia is usually made on the basis of the clinical history and radiographic findings. Clinical symptoms include fever, cough, and purulent sputum (10). It is important to note, however, that the signs and symptoms of pneumonia may be milder or even absent in the elderly (11). The etiology of pneumonia can be established from sputum, bronchoscopy specimens, blood culture, or fine-needle aspiration. Identification of the bacterial etiology from sputum specimens requires appropriate measures to ensure collection of good quality sputum specimen by avoiding contamination by upper airway flora (11). Unless these measures are taken, sputum Gram stain and culture have low sensitivity and specificity in the diagnosis (12). When purulent sputum uncontaminated by upper airway secretions can be obtained prior to the institution of antibiotics, sputum examination can have a sensitivity of up to 85% in the diagnosis of bacteremic pneumococcal pneumonia (13). Protected brush specimens obtained at bronchoscopy have a sensitivity of 50% to 80% (14,15) and a specificity >80% (14,16). Bronchoalveolar lavage (BAL), including protected lavage with quantitative culture of distal lung secretions, has a sensitivity and specificity similar to that of protected brush specimens (17,18). Blood cultures have poor sensitivity but a high specificity and are of prognostic importance in patients with pneumonia (11). Percutaneous fine-needle aspiration of the lung has only occasionally been used for the identification of pathogens in patients with pneumonia (19,20,21). In most cases when noninvasive techniques, such as sputum examination and cultures, are nondiagnostic, the patients are treated empirically. However, fine-needle biopsy may be useful in selected patients with aggressive nosocomial infections and in immunosuppressed patients (22,23). Positive cultures from needle aspiration have specificity and positive predictive value of 100%, but a relatively low sensitivity
and negative predictive values (approximately 60% to 70% and 30% to 40%, respectively) (23,24).
and negative predictive values (approximately 60% to 70% and 30% to 40%, respectively) (23,24).
Community-Acquired Pneumonia
The most commonly identified pathogen in community-acquired pneumonia is Streptococcus pneumoniae, which accounts for approximately 35% of identified organisms (25,26). Between 2% and 8% of patients have Haemophilus influenzae infection (27). Most of the remaining cases seen in the outpatient setting are caused by Mycoplasma pneumoniae, Chlamydia pneumoniae, and viruses (2,28,29). Anaerobic bacteria are an uncommon cause of community-acquired pneumonia. However, anaerobic bacteria have been isolated in approximately 20% to 35% of patients requiring hospitalization for pneumonia (30). Similarly, community-acquired Staphylococcus aureus pneumonia is uncommon and usually follows the influenza virus infection. However, S. aureus pneumonia is often associated with bacteremia and high mortality and should be considered in all severely ill patients admitted to the ICU for the management of pneumonia (31). Legionella species account for <2% of cases of pneumonia but its prevalence is higher in patients sick enough to require hospitalization and admission to the ICU (32). Gram-negative enteric organisms are an uncommon cause of community-acquired pneumonia, but should be considered in severely ill patients, especially those who are older, who have aspirated or who have significant underlying disease (33,34).
Nosocomial Pneumonia
Hospital-acquired (nosocomial) pneumonia is defined as pneumonia occurring 48 hours or more after admission (35). Bacteria are the most frequently identified cause. The most common organisms early in the hospital course (within the first 4 days) are S. pneumoniae, Moraxella catarrhalis, S. aureus, and H. influenzae (36). Most pneumonias that develop 5 or more days after hospitalization are caused by enteric gram-negative organisms, most commonly Enterobacter species, Escherichia coli, Klebsiella species, and Proteus species, or by S. aureus (35). Pneumonia is particularly common after surgery and in patients undergoing mechanical ventilation. Pneumonia may occur in up to 18% of patients who have undergone surgery (37) and up to 25% to 50% of patients undergoing mechanical ventilation (38,39,40). Nosocomial bacterial pneumonia is often difficult to recognize because the clinical criteria are nonspecific and bilateral areas of consolidation are often present secondary to acute respiratory distress syndrome (ARDS). In one investigation, nosocomial bacterial pneumonia was found histologically at autopsy in 58% of patients with ARDS, in 36% of whom it was unsuspected (41).
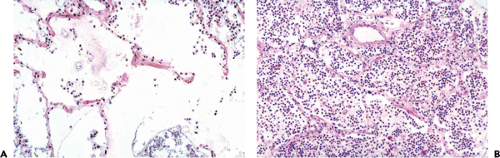 Figure 2.1 Lobar pneumonia. Photomicrographs show early (A) and advanced (B) stages of lobar pneumonia caused by Streptococcus pneumoniae. In (A), the airspaces are filled with edema fluid; only occasional neutrophils are evident. In (B), neutrophils predominate. The abundant fluid produced in the early stage of the disease flows relatively easily from airspace to airspace, resulting in the homogeneous consolidation seen grossly. Note that alveolar septa are intact in both stages of the disease, that is, there is no evidence of irreversible tissue damage. (From Müller NL, Fraser RS, Lee KS, et al. Diseases of the lung. Radiologic and pathologic correlations. Philadelphia, PA: Lippincott Williams & Wilkins; 2003.) |
The etiology of nosocomial pneumonia is influenced by the presence of specific risk factors. For example, anaerobic bacteria are more likely to be found in patients who develop pneumonia after aspiration or who have poor dentition or altered consciousness (42). Pseudomonas aeruginosa infection should be considered in patients who have received corticosteroids or broad-spectrum antibiotics, who have had a prolonged stay in the ICU, or who have underlying bronchiectasis (43). Prolonged hospitalization or prior use of antibiotics also favors the development of nosocomial pneumonia caused by antibiotic-resistant organisms, such as methicillin-resistant S. aureus, Acinetobacter species, Serratia marcescens, and P. aeruginosa (44).
Radiologic Manifestations of Bacterial Pulmonary Infection
Bacterial pulmonary infection is usually acquired through the tracheobronchial tree, most commonly by aspiration
or inhalation of microorganisms, or, occasionally, by direct physical implantation from an infected source, such as a bronchoscope (45). Pulmonary infection may also occur through the pulmonary vasculature, typically in association with an extrapulmonary focus of infection such as endocarditis. The organisms responsible for the infection may be found free in the blood (sepsis) or may be associated with thrombus (septic emboli).
or inhalation of microorganisms, or, occasionally, by direct physical implantation from an infected source, such as a bronchoscope (45). Pulmonary infection may also occur through the pulmonary vasculature, typically in association with an extrapulmonary focus of infection such as endocarditis. The organisms responsible for the infection may be found free in the blood (sepsis) or may be associated with thrombus (septic emboli).
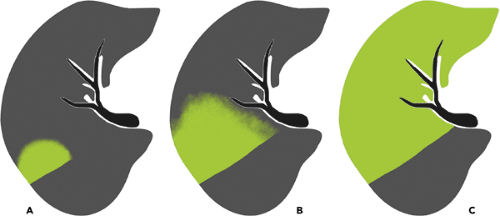 Figure 2.2 Progression of consolidation in lobar pneumonia. The consolidation usually occurs initially in the periphery of the lung adjacent to the visceral pleura or interlobar fissure (A). The infection spreads across segmental boundaries to occupy a confluent portion of the parenchyma (B). The area of consolidation abutting an interlobar fissure is sharply defined. The margins of the consolidation spreading to the remaining parenchyma tend to have ill-defined margins (ground-glass opacities on computed tomography scan) because the pneumonia initially results in only partial filling of the airspaces. The bronchi usually remain patent, resulting in an air bronchogram (C). (Courtesy of C. Isabela S. Silva, MD, PhD.) |
Bacteria result in two main types of pneumonia: Lobar (nonsegmental) pneumonia and bronchopneumonia (lobular pneumonia). Other manifestations include abscess formation, pneumatocele, septic embolism, pleural effusion, and empyema.
Lobar (nonsegmental) pneumonia is characterized histologically by the filling of alveolar airspaces by an exudate of edema fluid and neutrophils (see Fig. 2.1) (46). The consolidation usually begins in the periphery of the lung adjacent to the visceral pleura and spreads centripetally through interalveolar pores (pores of Kohn) and small airways (46). The airspace filling typically extends across pulmonary segments (nonsegmental consolidation), sometimes to involve the entire lobe (see Fig. 2.2). Lobar pneumonia is characterized on the radiograph and on computed tomography (CT) scan by the presence of homogeneous airspace consolidation involving adjacent segments of a lobe (see Fig. 2.3 and Table 2.1). The consolidation tends to occur initially in the periphery of the lung beneath the visceral pleura and usually abuts an interlobar fissure. The consolidation spreads centrally across segmental boundaries and may eventually involve the entire lobe. The bronchi usually remain patent, resulting in air bronchograms within the areas of consolidation. On high-resolution CT scan, areas of ground-glass opacities denoting incomplete filling of alveoli can often be seen adjacent to the airspace consolidation (see Fig. 2.4) (47,48). Most cases of lobar pneumonia are caused by bacteria, most commonly by S. pneumoniae and less commonly by Klebsiella pneumoniae, Legionella pneumophila, H. influenzae, and M. Tuberculosis (11,49).
Bronchopneumonia (lobular pneumonia) is characterized histologically by predominantly peribronchiolar inflammation (see Fig. 2.5) (46). This peribronchiolar inflammation is initially reflected by the presence of a small nodular or reticulonodular pattern on the radiograph and centrilobular nodules and branching opacities (tree-in-bud pattern) on high-resolution CT scan (see Fig. 2.6). Further extension into the adjacent parenchyma results in patchy airspace nodules (centrilobular lesions with poorly defined margins measuring 4 to 10 mm in diameter) (see Figs. 2.6 and 2.7) (46,50,51). These small foci of disease may
progress to lobular, subsegmental, or segmental areas of consolidation (see Figs. 2.6 and 2.8 and Table 2.2). The areas of consolidation may be patchy or confluent, involve one or more segments of a single lobe, and may be multilobar, unilateral, or bilateral (51). Confluence of pneumonia in adjacent lobules and segments may result in a pattern simulating lobar pneumonia; distinction from the latter can be made in most cases by the presence of segmental or lobular distribution of the abnormalities in other areas. Cavitation is common particularly in patients with extensive consolidation (22). Because it involves the airways, bronchopneumonia frequently results in loss of volume of the affected segments or lobes. Air bronchograms are seldom evident on the radiograph but can frequently be seen on high-resolution CT scan.
progress to lobular, subsegmental, or segmental areas of consolidation (see Figs. 2.6 and 2.8 and Table 2.2). The areas of consolidation may be patchy or confluent, involve one or more segments of a single lobe, and may be multilobar, unilateral, or bilateral (51). Confluence of pneumonia in adjacent lobules and segments may result in a pattern simulating lobar pneumonia; distinction from the latter can be made in most cases by the presence of segmental or lobular distribution of the abnormalities in other areas. Cavitation is common particularly in patients with extensive consolidation (22). Because it involves the airways, bronchopneumonia frequently results in loss of volume of the affected segments or lobes. Air bronchograms are seldom evident on the radiograph but can frequently be seen on high-resolution CT scan.
Table 2.1 Lobar (Nonsegmental) Pneumonia | |
|---|---|
|
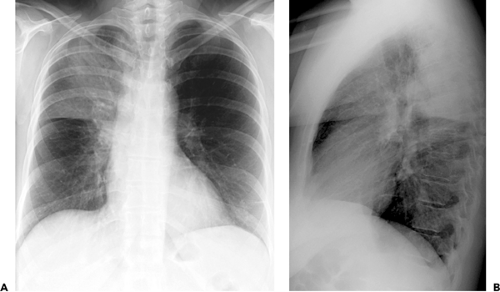 Figure 2.3 Lobar pneumonia. Posteroanterior (A) and lateral (B) chest radiographs show extensive consolidation in the right upper lobe. The consolidation crosses segmental boundaries, has well-defined margins where it abuts the interlobar fissures and poorly defined margins elsewhere. The patient was a 50-year-old woman with pneumococcal pneumonia. |
Characteristic manifestations of bronchopneumonia on high-resolution CT scan include centrilobular nodules and branching linear opacities, airspace nodules, and multifocal lobular areas of consolidation (see Fig. 2.9) (46,47,48). The nodular and branching linear opacities result in an appearance resembling a tree-in-bud and reflect the presence of inflammatory exudate in the lumen and walls of membranous and respiratory bronchioles and the lung parenchyma immediately adjacent to them (46). The nodules seen in bronchopneumonia usually measure 4 to 10 mm in diameter and have poorly defined margins. Although these nodular opacities are often referred to as “acinar shadows,” they reflect the presence of peribronchiolar areas of consolidation and not acinar consolidation (46,50). Therefore the term airspace nodules is preferable. The most common causative organisms of bronchopneumonia are S. aureus, H. influenzae, P. aeruginosa, and anaerobic bacteria (11,22,47).
It should be noted that the radiologic pattern is influenced by the presence of underlying disease such as emphysema and age, and immunologic status of the patient (52). It is also important to keep in mind that the radiographic manifestations are often delayed. This is particularly important in nosocomial infections in patients whose chest radiographs are often performed within hours of the onset of symptoms, a time when the pneumonia may not yet be apparent on the radiograph (22). Radiographic abnormalities may be particularly delayed in patients with neutropenia (53). In one study of 175 consecutive patients with gram-negative pneumonia who were neutropenic following antineoplastic chemotherapy, 70 episodes of pneumonia were initially diagnosed clinically, in the absence of radiographically detectable disease (53). In 27 of these 70 episodes, pneumonia was evident on a follow-up radiograph. In 25 of 57 patients with no radiographically detectable infiltrates, the diagnosis of pneumonia was established at autopsy (53). The radiographic appearance of a visible pneumonic infiltrate may be delayed not only in patients with neutropenia but also in those with functional defects of granulocytes due to diabetes, alcoholism, and uremia (22). CT scan, particularly high-resolution CT scan, has been shown to be more sensitive than the radiograph in the detection of subtle abnormalities and may show findings suggestive of pneumonia up to 5 days earlier than chest radiographs (54).
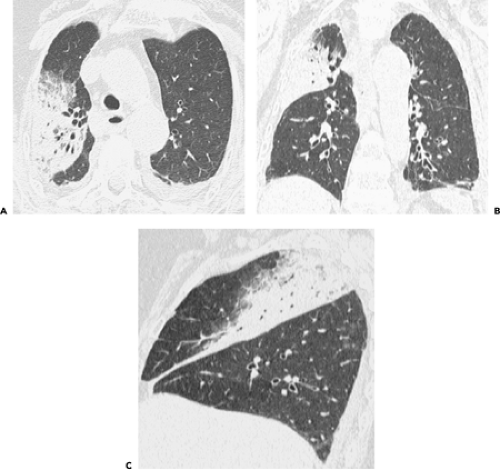 Figure 2.4 Lobar pneumonia. High-resolution computed tomography (CT) scan (1-mm collimation) (A) obtained in a multidetector CT scanner shows airspace consolidation in the right upper lobe. Note the presence of patent bronchi within the consolidation (air bronchogram) and the presence of ground-glass opacities at the boundary of the consolidation and normal lung. Coronal (B) and sagittal (C) reformations show that the consolidation crosses segmental boundaries and involves the apical, posterior and, to a lesser extent, anterior segments of the right upper lobe. |
High-resolution CT scan allows a better depiction of the pattern and distribution of pneumonia than the radiograph (48,55) but is seldom required in the evaluation of patients with suspected or proved bacterial pneumonia. CT scan is recommended, however, in patients with clinical suspicion of infection and normal or nonspecific radiographic findings, in the assessment of suspected complications of pneumonia or suspicion of an underlying lesion such as pulmonary carcinoma (22,56). CT scan is also indicated in patients with pneumonia and persistent or recurrent pulmonary opacities (22).
Lung abscess is defined as a localized necrotic cavity containing pus (57). It usually represents an inflammatory mass, the central part of which has undergone purulent liquefactive necrosis (11). The most common cause of lung abscess is aspiration (57). Abscesses occur most commonly in the posterior segment of an upper lobe or the superior segment of a lower lobe (57). However, they may also be present predominantly or exclusively in the anterior lung regions (see Fig. 2.10). Lung abscesses usually measure 2 to 6 cm in diameter, although they may become larger measuring up to 12 cm in diameter (57). Abscesses often
erode into an airway, resulting in drainage of necrotic material and the formation of a cavity (see Fig. 2.10). Pulmonary abscesses may develop in the course of known pneumonia or may be the initial manifestation of the disease. The radiologic manifestations consist of single or multiple masses that are often cavitated (see Table 2.3). In one review of the radiographic findings in 50 patients, the internal margins of the abscesses were smooth in 88% and shaggy in 12% (58). Air–fluid levels were present in 72% and adjacent parenchymal consolidation in 48%. Maximal wall thickness was equal to or <4 mm in 4% of cases, between 5 and 15 mm in 82%, and >15 mm in 14%. CT scan typically demonstrates low-attenuation central region or cavitation and rim enhancement following intravenous administration of contrast (Fig. 2.10) (59,60). Common causes of lung abscess include anaerobic bacteria (most commonly Fusobacterium nucleatum and Bacteroides species), S. aureus, P. aeruginosa, and K. pneumoniae (57,61).
erode into an airway, resulting in drainage of necrotic material and the formation of a cavity (see Fig. 2.10). Pulmonary abscesses may develop in the course of known pneumonia or may be the initial manifestation of the disease. The radiologic manifestations consist of single or multiple masses that are often cavitated (see Table 2.3). In one review of the radiographic findings in 50 patients, the internal margins of the abscesses were smooth in 88% and shaggy in 12% (58). Air–fluid levels were present in 72% and adjacent parenchymal consolidation in 48%. Maximal wall thickness was equal to or <4 mm in 4% of cases, between 5 and 15 mm in 82%, and >15 mm in 14%. CT scan typically demonstrates low-attenuation central region or cavitation and rim enhancement following intravenous administration of contrast (Fig. 2.10) (59,60). Common causes of lung abscess include anaerobic bacteria (most commonly Fusobacterium nucleatum and Bacteroides species), S. aureus, P. aeruginosa, and K. pneumoniae (57,61).
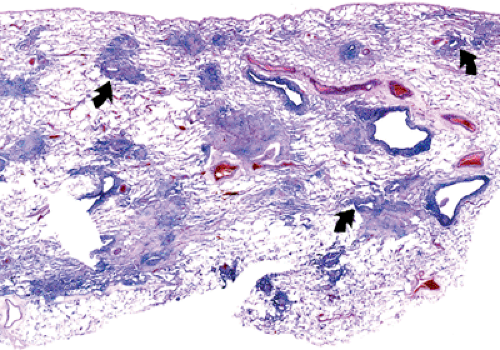 Figure 2.5 Acute bronchopneumonia. Low magnification photomicrograph shows several small foci of consolidation located around the lumens of small bronchioles (arrows). (From Müller NL, Fraser RS, Lee KS, et al. Diseases of the lung. Radiologic and pathologic correlations. Philadelphia, PA: Lippincott Williams & Wilkins; 2003.) |
 Figure 2.6 Progression of bronchopneumonia. The organisms may initially involve mainly the bronchioles resulting in centrilobular nodules and branching opacities (tree-in-bud pattern) (A). The consolidation initially involves the peribronchiolar regions. It progresses to become lobular, subsegmental or segmental (B and C). It is usually multifocal and patchy but the consolidation typically does not cross segmental boundaries. (Courtesy of C. Isabela S. Silva, MD, PhD.) |
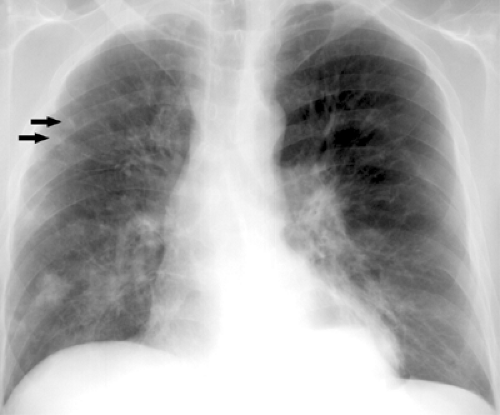 Figure 2.7 Bronchopneumonia. Chest radiograph shows poorly defined nodular opacities (arrows) in the right upper lobe and small bilateral foci of consolidation. Also noted is a large hiatus hernia with an air–fluid level. The patient was a 37-year-old man with Escherichia coli pneumonia. |
Occasionally pneumonia may result in extensive necrosis (necrotizing pneumonia). Radiologic manifestations
consist initially of small lucencies within an area of consolidated lung, usually developing within lobar consolidation associated with enlargement of the lobe and outward bulging of the fissure (bulging fissure sign) (62) (see Fig. 2.11). The lucencies rapidly coalesce into a large cavity containing fluid and sloughed lung (see Fig. 2.12).
consist initially of small lucencies within an area of consolidated lung, usually developing within lobar consolidation associated with enlargement of the lobe and outward bulging of the fissure (bulging fissure sign) (62) (see Fig. 2.11). The lucencies rapidly coalesce into a large cavity containing fluid and sloughed lung (see Fig. 2.12).
 Figure 2.8 Bronchopneumonia. Chest radiograph shows areas of consolidation in the right upper and left lower lobes. The patient was a 23-year-old man with bronchopneumonia. |
Pneumatocele is a thin-walled, gas-filled space that usually develops in association with infection (11). It presumably results from drainage of a focus of necrotic lung parenchyma followed by check-valve obstruction of the airway subtending it, enabling air to enter the parenchymal space during inspiration but preventing its egress during expiration (63). The complication is caused most often by S. aureus in infants and children and Pneumocystis jiroveci in patients who have acquired immunodeficiency syndrome (AIDS) (52,64). Pneumatoceles typically increase in size over days or weeks, may result in pneumothorax, and usually resolve over weeks or months (see Fig. 2.13).
Table 2.2 Bronchopneumonia (Lobular Pneumonia) | ||
|---|---|---|
|
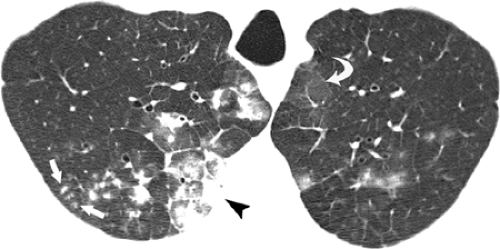 Figure 2.9 Bronchopneumonia. High-resolution computed tomography (CT) scan shows centrilobular nodules (arrows) and lobular areas of consolidation (arrowhead) and ground-glass opacity (curved arrow). The patient was a 53-year-old man with bronchopneumonia. |
Septic emboli to the lungs originate in a variety of sites, including cardiac valves (endocarditis), peripheral veins (thrombophlebitis), and venous catheters or pacemaker wires. The common feature in all these sites is endothelial damage associated with the formation of friable thrombus-containing organisms (usually bacteria) (52). Turbulence of flowing blood results in the detachment of small fragments of thrombus that are carried to the pulmonary arteries. Septic embolism is characterized radio-logically by the presence of nodules that usually measure 1 to 3 cm in diameter and that are frequently cavitated (see Fig. 2.14). The cavitation reflects the necrosis associated with the organisms and the neutrophilic exudate. On cross-sectional CT images the nodules often appear to have a vessel leading into them. This has been called the feeding vessel (see Fig. 2.15) (65,66). Multiplanar and maximum intensity projection (MIP) reformations have shown however that in most patients the pulmonary arteries course around the nodule and that vessels appearing to enter the nodule usually are pulmonary veins draining the nodule (Fig. 2.15) (67). Dodd et al. performed multidetector high-resolution CT scan in 14 patients with septic embolism (67). Ninety-three nodules (40%) showed a vessel that appeared to enter the nodule on transverse images, but the vessel was shown to pass around the nodule on multiplanar reconstructions and/or MIPs. Forty-four nodules (19%) showed a central vessel entering the lesion on all imaging planes. All of these vessels could be traced back to the left atrium on transverse images, consistent with pulmonary vein branches. The “feeding vessel” sign is therefore a misnomer and is of limited value in the diagnosis of septic embolism.
Occlusion of pulmonary arteries by septic emboli or thrombus may result in hemorrhage and/or infarction and less well-defined or wedge-shaped foci of disease. These subpleural wedge-shaped areas of consolidation,
often with central areas of necrosis or frank cavitation, are often difficult to identify on the radiograph but are commonly seen on CT scan (66). Septic emboli are seen most commonly in intravenous drug users and in patients with central venous lines.
often with central areas of necrosis or frank cavitation, are often difficult to identify on the radiograph but are commonly seen on CT scan (66). Septic emboli are seen most commonly in intravenous drug users and in patients with central venous lines.
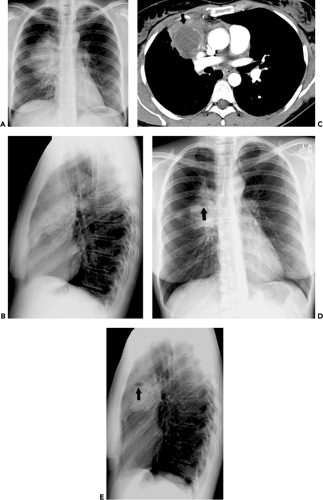 Figure 2.10 Lung abscess. Posteroanterior (A) and lateral (B) chest radiographs show dense right upper airspace consolidation. Contrast-enhanced computed tomography (CT) scan (C) demonstrates large focal area of decreased attenuation with rim enhancement (arrow) characteristic of lung abscess. Posteroanterior (D) and lateral (E) chest radiographs 3 weeks later show decreased size of lung abscess and development of cavitation with fluid level (arrows). The patient was a 43-year-old woman with lung abscess secondary to Haemophilus aphrophilus. |
Table 2.3 Lung Abscess | ||
|---|---|---|
|
Aerobic Bacteria
Gram-positive Cocci
Streptococcus Pneumoniae
S. pneumoniae (pneumococcus) is the most commonly identified pathogenic organism in patients admitted to the hospital for pneumonia, accounting for approximately 40% of all isolated species (27,68). Risk factors for the development of pneumococcal pneumonia include the extremes of age (69,70,71), chronic heart or lung disease (70,71), immunosuppression (70,71), alcoholism (72), institutionalization (73,74), and prior splenectomy (75). The characteristic clinical presentation is abrupt in onset, with fever, chills, cough, and pleuritic chest pain. In the elderly, these classic features of disease may be absent, and pneumonia may be confused with or confounded by other common medical problems, such as congestive heart failure, pulmonary thromboembolism, or malignancy (74,76).
 Figure 2.11 Bulging fissure sign. Posteroanterior chest radiograph shows dense right upper lobe airspace consolidation with downward bulging of the minor fissure. The patient was a 66-year-old man with pneumococcal pneumonia. |
The characteristic radiographic pattern of acute pneumococcal pneumonia consists of homogeneous consolidation that crosses segmental boundaries (nonsegmental) but involves only one lobe (lobar pneumonia) (see Figs. 2.16 and 2.17 and Table 2.4) (11). Because the consolidation begins in the peripheral airspaces of the lung, it almost invariably abuts against a visceral pleural surface, either interlobar or over the convexity of the lung (11). Occasionally, infection is manifested as a spherical focus of consolidation that simulates a mass (round pneumonia); this pattern is seen more commonly in children than in adults (see Fig. 2.18) (77).
Although homogeneous lobar consolidation is the most characteristic radiographic manifestation of acute pneumococcal pneumonia, other patterns are not uncommon. In one prospective study of 30 patients with S. pneumoniae, 20 (67%) had lobar consolidation (lobar pneumonia), 6 (20%) had patchy areas of consolidation (bronchopneumonia), and 4 (13%) had mixed airspace and reticulonodular opacities (see Figs. 2.19 and 2.20) (78). In another review of 132 patients who had severe community-acquired pneumonia treated in the ICU, 28 (65%) of 43 patients with S. pneumoniae pneumonia had typical lobar consolidation, and 35% had bronchopneumonia; none had reticular or reticulonodular opacities (79).
Complications, such as cavitation and pneumatocele formation, are rare. It is probable that many of these are related to mixed infections; associated anaerobic microorganisms in particular are likely to be undetected because of lack of appropriate culture methods (80). Pleural effusion is evident on posteroanterior and lateral radiographs in approximately 10% of patients overall (81); effusion is present in approximately 30% of patients who have severe pneumonia requiring treatment in the ICU (79), and in 50% of patients with bacteremia (82). Lymphadenopathy is seldom evident on the radiograph but is commonly seen on CT scan (83). In one study of 35 adults hospitalized with pneumococcal pneumonia, intrathoracic lymphadenopathy was present on CT scan in 19 (54%) patients (83). The lymphadenopathy was ipsilateral to the pneumonia in 100% of patients (19 of 19 patients). One patient also had contralateral lymphadenopathy. Comorbidities included HIV infection (n = 15); smoking (n = 21); emphysema (n = 5); hepatitis C (n = 5); and diabetes (n = 3). None of the differences in the prevalence of lymphadenopathy among the subgroups was statistically significant.
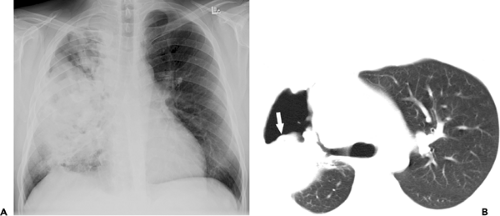 Figure 2.12 Necrotizing pneumonia. Chest radiograph (A) shows inhomogeneous and dense consolidation in the right lung. Computed tomography (CT) (B) image shows a large cavity and sloughed lung within the cavity (arrow). The patient was a 42-year-old alcoholic man with necrotizing pneumonia secondary to Klebsiella pneumoniae and anaerobic organisms. |
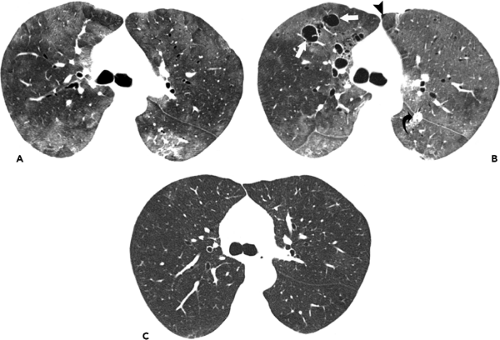 Figure 2.13 Pneumatoceles. High-resolution computed tomography (CT) image at the level of the main bronchi (A) shows extensive bilateral ground-glass opacities. High-resolution CT scan image at the same level 1 month later (B) shows several pneumatoceles (straight arrows) in the right upper lobe. Also noted is a small left pneumothorax (arrowhead) and a left chest tube in the major fissure (curved arrow). The patient was a 55-year-old woman who developed Pneumocystis pneumonia while undergoing treatment for nonHodgkin lymphoma. The pneumonia resolved but no follow-up images immediately following resolution of the pneumonia were available. High-resolution CT scan image 3 years later (C) demonstrates resolution of the pneumatoceles. |
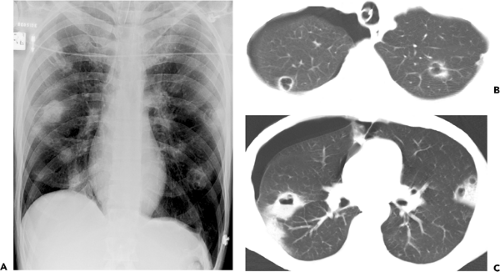 Figure 2.14 Septic embolism. Posteroanterior chest radiograph (A) shows several bilateral cavitating nodules. Computed tomography (CT) images (5-mm collimation) at the level of the upper (B) and middle (C) lung zones demonstrate that the cavitating nodules are located mainly in the subpleural lung regions. Also noted is a small right pneumothorax. |
CT scan seldom adds any clinically relevant information in patients with characteristic radiographic and clinical findings of pneumococcal pneumonia and therefore is seldom warranted in these patients. CT scan is helpful, however, in patients with suspected complications such as cavitation, empyema, and bronchopleural fistula. Donnelly et al. performed contrast-enhanced CT scans in 56 children with complicated pneumonia of various etiologies (84). CT scans were evaluated for clinically significant findings that were not revealed by radiography including lung parenchymal complications (cavitary necrosis, abscess, bronchopleural fistula), pleural complications (loculation, malpositioned chest tube), inaccurate estimation of cause of chest opacity on radiography (pleural vs. parenchymal), bronchial obstruction, or pericardial effusion. A total of 110 CT scan findings, not revealed by radiography,
were seen including 40 parenchymal complications, 37 pleural complications, 20 inaccurate estimations of cause of chest opacity on radiography, and 13 pericardial effusions. All CT scans showed at least one significant finding not seen on radiography (84). Hodina et al. reviewed the radiographs and CT scan images of nine children admitted in the pediatric ICU for persistent or progressive pneumonia, respiratory distress, or sepsis despite adequate antibiotic therapy, including four patients with S. pneumoniae pneumonia (85). Chest radiographs showed consolidations in eight of the nine patients. On CT scan examination, cavitary necrosis was localized to one lobe in two patients, and seven patients showed multilobar or bilateral areas of cavitary necrosis. In three of the nine patients the cavitary necrosis was initially shown on CT scan and visualization by chest radiography was delayed by a time span varying from 5 to 9 days. Parapneumonic effusions were shown by chest radiography in three patients and by CT scan in five patients. Bronchopleural fistulae, present in three patients, were only seen on CT scan. The authors concluded that CT scan allows a better assessment of the presence of pulmonary and pleural complications in children with necrotizing pneumonia and allows an earlier diagnosis of this rapidly progressing condition (85).
were seen including 40 parenchymal complications, 37 pleural complications, 20 inaccurate estimations of cause of chest opacity on radiography, and 13 pericardial effusions. All CT scans showed at least one significant finding not seen on radiography (84). Hodina et al. reviewed the radiographs and CT scan images of nine children admitted in the pediatric ICU for persistent or progressive pneumonia, respiratory distress, or sepsis despite adequate antibiotic therapy, including four patients with S. pneumoniae pneumonia (85). Chest radiographs showed consolidations in eight of the nine patients. On CT scan examination, cavitary necrosis was localized to one lobe in two patients, and seven patients showed multilobar or bilateral areas of cavitary necrosis. In three of the nine patients the cavitary necrosis was initially shown on CT scan and visualization by chest radiography was delayed by a time span varying from 5 to 9 days. Parapneumonic effusions were shown by chest radiography in three patients and by CT scan in five patients. Bronchopleural fistulae, present in three patients, were only seen on CT scan. The authors concluded that CT scan allows a better assessment of the presence of pulmonary and pleural complications in children with necrotizing pneumonia and allows an earlier diagnosis of this rapidly progressing condition (85).
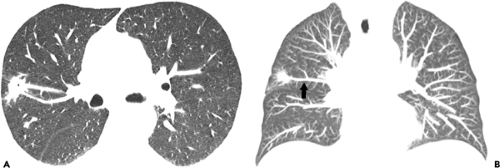 Figure 2.15 Feeding vessel sign. Cross-sectional high-resolution computed tomography (CT) image (A) shows two vessels apparently coursing into a nodule (“feeding vessel sign”). Coronal maximum intensity projection image (B) demonstrates that the only vessel in close contact with the nodule is a draining vein (arrow). |
 Figure 2.16 Lobar pneumonia due to Streptococcus pneumoniae. Chest radiograph shows nonsegmental right upper lobe consolidation. The patient was a 71-year-old man with pneumococcal pneumonia. |
Staphylococcus Aureus
S. aureus is an uncommon cause of community-acquired pneumonia, accounting for only approximately 3% of all cases (25,26,27). It is, however, an important cause of nosocomial pneumonia, especially in the ICU. In this setting, S. aureus is one of the more common pathogenic organisms, being found in 15% or more of all cases (86,87,88,89). Of particular importance is the dramatic increase of the incidence of methicillin-resistant Staphylococcus aureus (MRSA) infections in recent years in patients admitted to the ICU and the associated increase in morbidity and mortality (90).
Bacteremic S. aureus pneumonia is found most commonly in ICU patients and in intravenous drug users (91). In one prospective study of 134 cases, 80% of primary staphylococcal pneumonias were nosocomial and 68% of the overall cases were in patients in the ICU; 72% of the patients with community-acquired S. aureus pneumonia were intravenous drug users (91).
The clinical presentation of S. aureus pneumonia usually is abrupt, with fever, pleuritic chest pain, cough, and expectoration of purulent yellow or brown sputum, sometimes streaked with blood (11). The characteristic pattern of presentation pathologically and radiologically is as a bronchopneumonia (lobular pneumonia) (see Table 2.5) (46). S. aureus bronchopneumonia, like other bronchopneumonias, is characterized histologically by predominantly peribronchiolar inflammation (46). This results in poorly defined 4 to 10 mm-diameter nodules (airspace nodules) (see Fig. 2.21). The airway involvement in S. aureus bronchopneumonia is easier to see on high-resolution CT scan than on the radiograph (92). It is manifested on high-resolution CT scan by centrilobular nodular and branching
linear opacities (tree-in-bud pattern) seen in approximately 40% of patients with staphylococcal pneumonia (see Fig. 2.22) (47,92). The peribronchiolar inflammation usually progresses rapidly to lobular, subsegmental, or segmental areas of consolidation, which may be patchy or confluent. The pneumonia is bilateral in approximately 40% of patients. Depending on the severity of involvement, the process may be patchy or homogeneous; the latter represents confluent bronchopneumonia (see Fig. 2.23). Because an inflammatory exudate fills the airways, segmental atelectasis may accompany the consolidation, and air bronchograms are seldom evident on the radiograph (46).
linear opacities (tree-in-bud pattern) seen in approximately 40% of patients with staphylococcal pneumonia (see Fig. 2.22) (47,92). The peribronchiolar inflammation usually progresses rapidly to lobular, subsegmental, or segmental areas of consolidation, which may be patchy or confluent. The pneumonia is bilateral in approximately 40% of patients. Depending on the severity of involvement, the process may be patchy or homogeneous; the latter represents confluent bronchopneumonia (see Fig. 2.23). Because an inflammatory exudate fills the airways, segmental atelectasis may accompany the consolidation, and air bronchograms are seldom evident on the radiograph (46).
Table 2.4 Streptococcus Pneumoniae (Pneumococcal) Pneumonia | ||
|---|---|---|
|
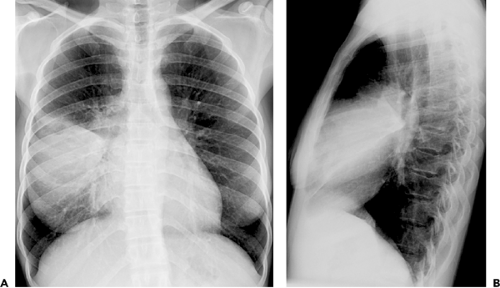 Figure 2.17 Lobar pneumonia due to Streptococcus pneumoniae. Posteroanterior (A) and lateral (B) chest radiographs show extensive right middle lobe consolidation. The patient was a 29-year-old woman with pneumococcal pneumonia. |
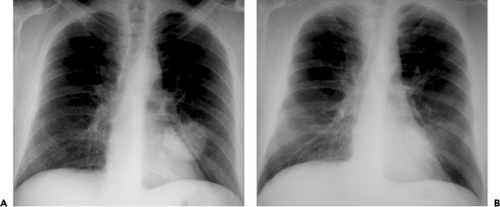 Figure 2.18 Round pneumonia due to Streptococcus pneumoniae. Chest radiograph (A) shows a round area of consolidation mimicking a mass in the left lower lobe. Chest radiograph 1 week later (B) shows almost complete resolution of the airspace consolidation. The patient was a 50-year-old man with pneumococcal pneumonia. |
In a review of the radiographic abnormalities of 26 adults with community-acquired staphylococcal pneumonia, 14 (54%) had homogeneous consolidation, 12 (46%) had patchy consolidation, and 2 (8%) had a mixed picture (51). The consolidation involved a single lobe
in 36% of cases, more than one lobe in 54%, and was bilateral in 35%. In a second series of 31 adults, 15 (60%) had multilobar consolidation and 12 (39%) had bilateral pneumonia (93); the consolidation involved predominantly or exclusively the lower lobes in 16 patients (64%). Abscesses develop in 15% to 30% of patients (51,93). The abscesses are usually solitary and typically have an irregular shaggy inner wall. Pneumatocele formation also is common, occurring in approximately 50% of children (94) and 15% of adults (51). Pneumatoceles usually appear during the first week of the pneumonia and disappear spontaneously within weeks (95) or months (96). Spontaneous pneumothorax, which is presumably secondary to ruptured pneumatoceles, occurs in approximately 10% of adults and 30% of children (51). Pleural effusions occur in 30% to 50% of patients; of these, approximately half represent empyemas (see Fig. 2.24) (51,93).
in 36% of cases, more than one lobe in 54%, and was bilateral in 35%. In a second series of 31 adults, 15 (60%) had multilobar consolidation and 12 (39%) had bilateral pneumonia (93); the consolidation involved predominantly or exclusively the lower lobes in 16 patients (64%). Abscesses develop in 15% to 30% of patients (51,93). The abscesses are usually solitary and typically have an irregular shaggy inner wall. Pneumatocele formation also is common, occurring in approximately 50% of children (94) and 15% of adults (51). Pneumatoceles usually appear during the first week of the pneumonia and disappear spontaneously within weeks (95) or months (96). Spontaneous pneumothorax, which is presumably secondary to ruptured pneumatoceles, occurs in approximately 10% of adults and 30% of children (51). Pleural effusions occur in 30% to 50% of patients; of these, approximately half represent empyemas (see Fig. 2.24) (51,93).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


