6 Atrioventricular Septal Defect
Echocardiographic Assessment
Background
Key Points
Anatomy
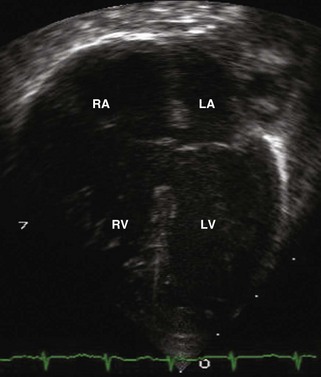
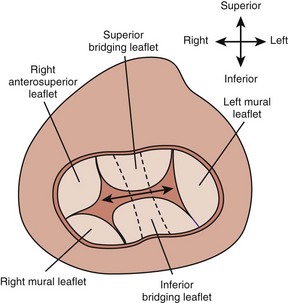
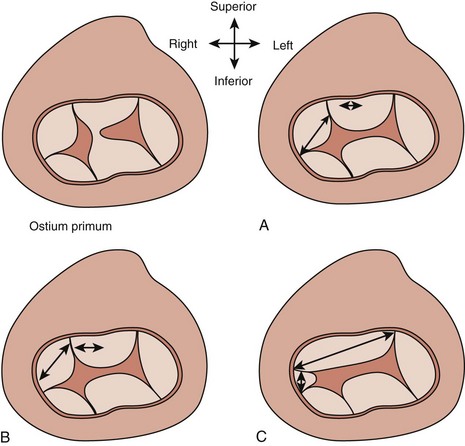
A complete AVSD has a common AV junction, a primum ASD, an IVSD, and a common AVV (Fig. 6-1). The primum ASD is anterior and inferior to the fossa ovalis, adjacent to the AVVs. The AVV consists of five leaflets: superior and inferior bridging leaflets, a left mural leaflet, a right mural leaflet, and a right anterosuperior leaflet (Fig. 6-2).
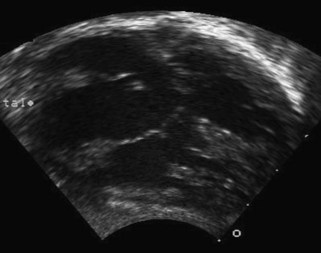
A partial AVSD usually has a primum ASD and two separate AVVs, with a cleft in the anterior leaflet of the left-sided AVV (mitral valve [MV]) (Fig. 6-3). The cleft in the left-sided AVV usually results in some degree of regurgitation of the valve. There are rare instances of partial AVSDs with only an IVSD and no primum ASD.

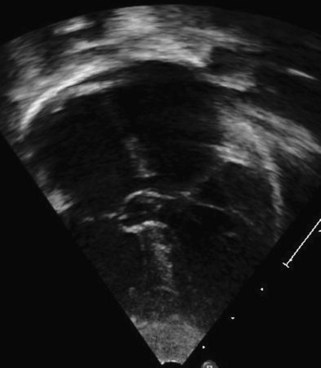
Figure 6-3 Parasternal short axis view showing a cleft in the anterior leaflet of the left-sided AVV.
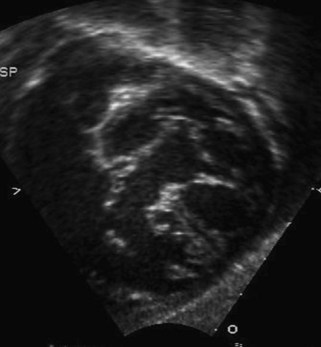
The term transitional AVSD has been used to refer to complete AVSDs in which the IVSD is predominantly occluded by chordal tissue from the AVV, resulting in minimal or no ventricular level shunting (Fig. 6-4). In transitional defects, there are two separate AVV orifices with a cleft in the left-sided AVV.
Overview of the Echocardiographic Approach
The echocardiogram (echo) should fully evaluate all the components of the AVSD and assess for any associated abnormalities. Images should define the size of the atrial and ventricular components and demonstrate the direction of shunting. The AVV attachments need to be defined, and function of the AVV should be assessed by pulsed wave (PW) Doppler and color flow Doppler (CFD). The balance of the AVV above the ventricles should be evaluated along with flow across the valve to demonstrate the flow into both ventricles. Additional ASDs or ventricular septal defects (VSDs) can be present, and careful assessment of the atrial septum (AS) and ventricular septum (VS) should be performed. The outflow tracts should be interrogated, looking for any obstruction (Box 6-1).
Goals of Echocardiographic Examination
AVSDs are described by Rastelli classification, which is based on papillary muscle configuration, specifically attachments of the superior bridging leaflet (Box 6-2 and Fig. 6-5):
Anatomic Imaging
Subcostal views allow evaluation of the primum ASD to determine size and direction of flow (Fig. 6-6). Subcostal short axis view allows an en face view of the AVV and can be used to assess the balance of the valve to the ventricles and look for attachments of the superior bridging leaflet to determine the Rastelli classification (Figs. 6-7 and 6-8).