Classification
Atrioventricular (AV) block is classified as first, second or third degree depending on whether conduction of atrial impulses to the ventricles is delayed, intermittently blocked or completely blocked.
First-degree atrioventricular block
Delay in conduction of the atrial impulse to the ventricles results in prolongation of the PR interval (Figures 15.1–15.3). The PR interval is measured from the onset of the P wave to the onset of the ventricular complex – whether this is a Q or an R wave – and is prolonged if it is greater than 0.21 s. Since conduction of the atrial impulse is only delayed, the term first-degree AV ‘block’ is, in fact, a misnomer.
First-degree AV block does not cause symptoms but may sometimes progress to higher degrees of block. In young people it is usually due to high vagal tone and is benign.

Figure 15.2 First-degree AV block and sinus tachycardia (lead I). PR interval = 0.24 s.

Figure 15.3 First-degree AV block (lead V1). The P wave is superimposed on the terminal portion of the preceding T wave. PR interval = 0.38 s.


Second-degree atrioventricular block
In second-degree AV block there is intermittent failure of conduction of atrial impulses to the ventricles. Thus, some P waves are not followed by QRS complexes.
Second-degree block is subdivided into Mobitz type I (also termed Wenckebach) and Mobitz type II block.
Mobitz type I (Wenckebach) atrioventricular block
In this form of second-degree block, delay in AV conduction increases with each successive atrial impulse until an atrial impulse fails to be conducted to the ventricles, i.e. there is progressive increase in PR interval until a P wave is not followed by a QRS complex. After the non-conducted P wave, AV conduction recovers and the sequence starts again (Figures 15.4, 15.5). Typically, the increments in PR interval progressively shorten during the sequence, resulting in progressive decrease in the interval between QRS complexes.
Figure 15.5 Wenckebach AV block. Unlike textbook examples, but as often occurs in practice, the trace does not start with the shortest PR interval.
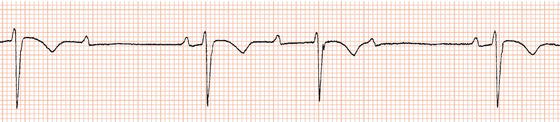
Figure 15.6 Mobitz type II AV block. In this example the ratio between conducted and non-conducted atrial impulses varies.


Wenckebach AV block is usually due to impaired conduction in the AV node. However, like first-degree AV block, it can be benign (particularly when it occurs during sleep), being due to high vagal tone. Wenckebach block that cannot be attributed to high vagal tone, e.g. in an older person during waking hours, has a prognosis similar to that of Mobitz type II block.
Unlike textbook examples, often in practice an ECG recording of AV Wenckebach block will not start with the shortest PR interval. If, at first glance, it is clear that there are non-conducted P waves but it is not obvious what type of AV block is occurring, ask yourself, ‘Is this Wenckebach block?’ Look for the shortest PR interval and then see if it progressively increases.
Mobitz type II atrioventricular block
In Mobitz type II block there is intermittent failure of conduction of atrial impulses to the ventricles without preceding progressive lengthening of the PR interval, and thus the PR interval of conducted beats is constant (Figure 15.6).
In contrast to first-degree and Wenckebach AV block, Mobitz type II block is usually due to impaired conduction in the bundle branches. Because there is bundle branch disease, the QRS complexes are as a rule broad (Figure 15.7). Block below the AV node is more likely to be associated with Stokes–Adams attacks, slow ventricular rates and sudden death.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


