Atrial Fibrillation and Shortness of Breath
A 42-year-old woman had her first episode of atrial fibrillation 3 years ago. Over the last year, she developed symptoms of fatigue and shortness of breath.
Physical examination showed no signs of cardiac decompensation. On auscultation, a split second heart sound was noted.
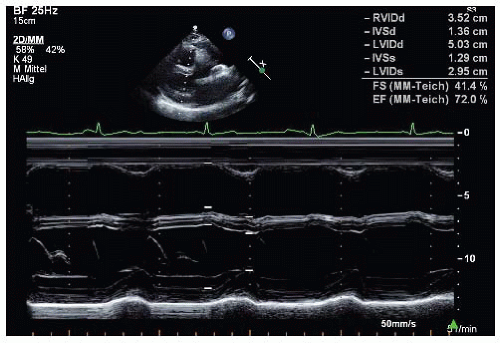 Figure 24-1. M-mode, parasternal long-axis view. |
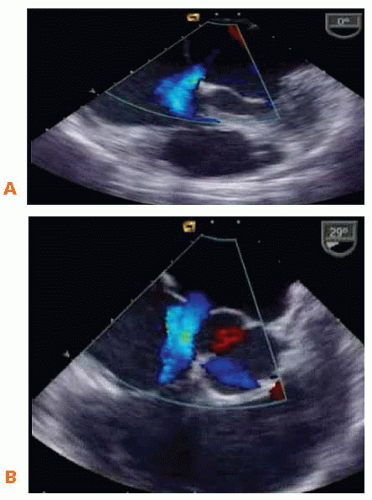 Figure 24-2. A. Conventional 2D transesophageal echocardiogram (TEE) with color Doppler in different planes at 0°. B. Conventional 2D TEE with color Doppler at 30°. |
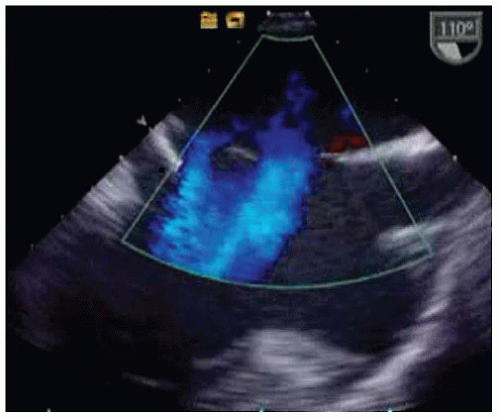 Figure 24-3. Conventional 2D TEE with and without color Doppler at 110°. |
QUESTION 1. What is the diagnosis?
A. Ventricular septal defect
B. Secundum atrial septal defect
C. Atrioventricular (AV) canal defect
D. Left-to-right shunting through a stretched patent foramen ovale
View Answer
ANSWER 1: B. The short-axis view (Fig. 24-2 and Video 24-1) at 30° shows that the patient had no aortic rim, and the long-axis view (Fig. 24-3 and Video 24-2) at 110° documents two atrial septal defects in the secundum portion of the atrial septum.
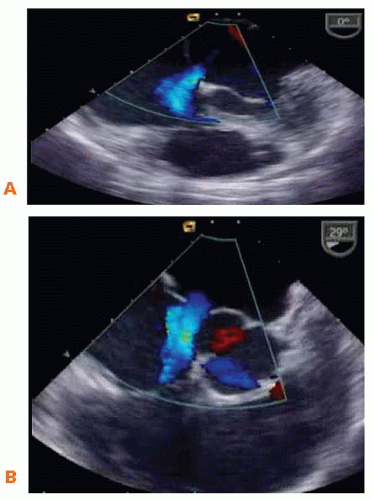 Figure 24-2. A. Conventional 2D transesophageal echocardiogram (TEE) with color Doppler in different planes at 0°. B. Conventional 2D TEE with color Doppler at 30°. |
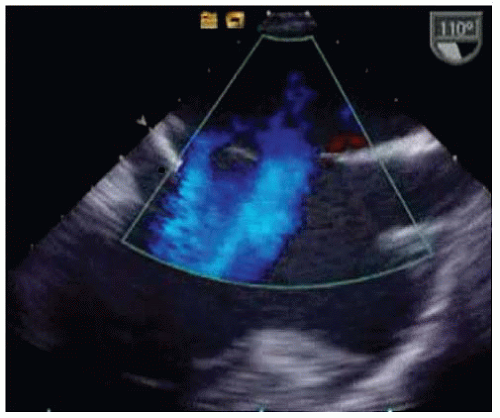 Figure 24-3. Conventional 2D TEE with and without color Doppler at 110°. |
QUESTION 2. How would you proceed?
A. The patient has only mild symptoms; a routine follow-up in 6 months is sufficient
B. Closure of the atrial septal defects (surgery or transcatheter closure)
View Answer




ANSWER 2: B. Indications for atrial septal defect closure include symptoms and/or right ventricular/right atrial enlargement and/or a pulmonic blood flow: Systemic blood flow > 1.5 and/or paradoxical embolism.1
The patient has symptoms, and the M-mode (Fig. 24-1) shows right ventricular enlargement.
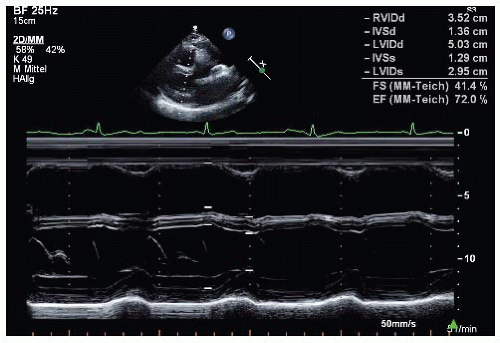 Figure 24-1. M-mode, parasternal long-axis view. |
Therefore, treatment is indicated, and it was decided to close the defect with percutaneous closure devices.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
